- 144 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
This accessible, jargon-free guide to uveitis for non-specialists explains in practical, easy-to-understand language how to diagnose and manage inflammatory eye disease. Describing in simple terms how to differentiate between the various inflammatory eye diseases, which investigations to choose, how to interpret the results and how best to manage immunosuppression in these patients, this book makes this fascinating subject accessible to the non-uveitis specialist for the first time.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
1 |
| Classification of uveitis |
The classification of uveitis is paramount to its understanding. Working out what is the cause of the disease, and hence how to treat it, is dependent on being able to classify it. Uveitis, inflammation of a portion or all of the uveal tract, can be classified according to the anatomical location of the inflammation, the severity and the course of the disease, and the cause of the uveitis. Classifying by cause is not so useful when seeing a patient for the first time and will not be discussed in detail here. Classifying by severity and course is useful but by far the most vital part of approaching a patient with inflammatory eye disease is knowing where the primary site of the inflammation is located, and whether one or both eyes are involved.
Classification by anatomical location
When a patient with an inflamed eye enters eye casualty the main filter that will guide you in diagnosing and treating the problem is the anatomical location of the primary site of the inflammation. The uveal tract, a highly vascularised pigmented layer of tissue located between the retina on the inside and the sclera on the outside, is split into three main parts (Figure 1.1). These consist of the iris anteriorly, the ciliary body immediately behind this forming a band 6 mm wide posterior to the iris root, with everything behind this forming the choroid.
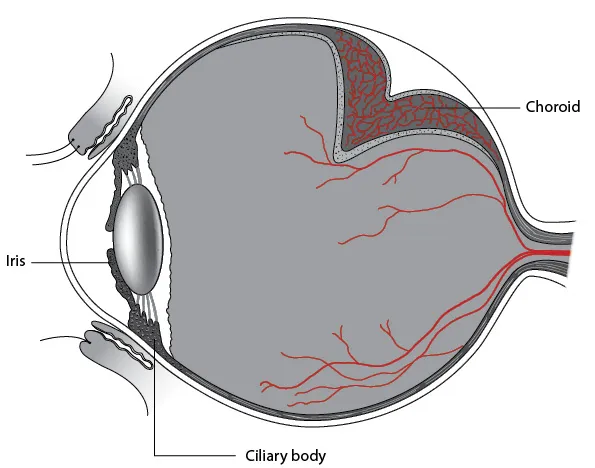
Figure 1.1Classification of uveitis by anatomy.
The inflammation may be primarily located in the iris, in which case the condition is called anterior uveitis, the ciliary body and vitreous, in which case the condition is called intermediate uveitis, or any ‘back of the eye structure’ such as the retina, retinal vessels or choroid, in which case posterior uveitis is the term. If all three are inflamed and it is not really possible to tell if one location is worse than any other then panuveitis is the term. Human tissue rarely gets inflamed in isolation of course and if one location is inflamed then it is common for surrounding tissues to be involved to a greater or lesser degree, in which case knowing which is the primary or most severely involved site is key. Anterior uveitis, for example, can spill over to the ciliary body and anterior vitreous to an extent although the signs are worse anteriorly. Likewise intermediate uveitis can have signs anteriorly and posteriorly as well so looking where the signs are most severe is time well spent in clinic and not doing this properly can lead to diagnostic errors. A fire in one building on a street can result in smoke pouring from not only the building on fire but some smoke escaping from those structures next door as well. Knowing where the smoke is densest will guide firefighters to where to direct their hoses and spraying all buildings without thought to where the main fire is will result in unnecessary water damage and delay in extinguishing the fire.
Just as inflammation can spread from one part of the uveal tract to another it can also spread inwardly and outwardly. To complicate things further the term ‘posterior uveitis’ is imprecisely and confusingly used to describe inflammation anywhere in the back of the eye and can occur with or without involvement of the choroid. For example, inflammation primarily involving the retina, retinitis, can occur either in isolation, without involvement of the choroid, or secondarily to inflammation in the choroid. Similarly, primary inflammation of the choroid can spread to involve the retina secondarily to cause a retinitis. The same is true for posterior spread to involve the outer coat, the sclera. Endophthalmitis is a condition where the entirety of the inside of the eye is inflamed such that the layer most affected cannot be discerned. In this condition the outermost coat, the sclera, is not yet heavily involved. Panophthalmitis is where the inside of the eye and all three coats are inflamed. Although strictly speaking the uveal tract is one distinct layer of the eye, the term ‘uveitis’ rather confusingly is often applied to any intraocular inflammation, in much the same way as ‘America’ can be a term applied to either the country or the continent.
Anterior uveitis, also called iritis as this is the portion of the uveal tract involved, is a very common condition to present to eye casualty. Again we state that the first thing one must do to determine what type of uveitis is present is to determine what anatomical locations are involved and where the primary source of the inflammation is located. This is highlighted as the most common error made that leads to uveitis specialists being called as expert witnesses in medicolegal cases where a posterior uveitis with mild anterior component is seen in eye casualty and treated with topical drops alone. This is almost always due to the casualty officer not dilating the pupil and looking at the fundus, and in turn this is almost always due to time pressure in accident and emergency resulting in corners being cut. If determining the primary source of the inflammation is paramount in working through diagnosis and treatment, this is impossible to do without actually looking at all the sites.
Tip: Always dilate patients presenting with anterior uveitis and examine the entire eye for inflammation. Always examine both eyes.
Classification by severity and course of the disease
The Standardisation of Uveitis Nomenclature (SUN) working group has established specific criteria for determining the severity of flare and cells in the anterior chamber and degree of vitritis in the posterior segment. These will be dealt with in their respective chapters. The course of the disease begins with the onset itself and knowing if this was sudden or insidious is important as it can help differentiate between conditions. If the episode lasts less than or equal to 3 months the duration is said to be limited and if greater than 3 months persistent. If there are multiple inflammatory episodes separated by more than or equal to 3 months without treatment the condition is said to be recurrent, but if the gap between episodes is less than 3 months it is called chronic (see Table 1.1).
Table 1.1Classification of uveitis by course of the disease
| Time | ≤3 months | >3 months |
| Duration | Limited | Persistent |
| Separation between episodes – the time between episodes of inflammation when the eye was quiet and the patient was on no treatment | Chronic | Recurrent |
Classification by cause of the disease
The purpose of classifying uveitis when first seeing a patient is to determine its cause. There are legion causes of uveitis which we will discuss as we get to them, but essentially these can be broken down into three categories: infectious, inflammatory and neoplasia mimicking inflammation. The term ‘masquerade syndrome’ is sometimes used to describe the latter as it presents in a number of ways although there are certain features that are constant and which the initiated can look out for. Clearly the treatment for all three is very different but until it is known for certain which of the three main causes is to blame some ba...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Contents
- Foreword
- Acknowledgement
- Authors
- Introduction
- 1. Classification of uveitis
- 2. Differentiating between different diagnoses: Clinical and ancillary testing
- 3. Anterior uveitis
- 4. Intermediate uveitis
- 5. Posterior uveitis
- 6. Panuveitis
- 7. Scleritis and episcleritis
- 8. Immunosuppression: Medications, and how to use and monitor them
- 9. Advanced therapies and future treatments
- 10. The moral ophthalmologist
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Practical Uveitis by Gwyn Samuel Williams,Mark Westcott in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over one million books available in our catalogue for you to explore.