eBook - ePub
The Foundations of Primary Care
v. 1, Satisfaction or Resentment?
- 240 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
This work contains foreword by Ian R McWhinney, Emeritus Professor of General Practice, Schulich School of Medicine and Dentistry, Centre for Studies in Family Medicine University of Western Ontario, Canada. This ground-breaking book encourages a re-focus on the subjective and social nature of health and illness. It helps healthcare professionals find fresh perspectives to assist patients, many of whom are threatened by and lost in a healthcare system dominated by diseases and procedures. The book takes a whole systems approach to primary care, incorporating new developments, social aspects, critical discourse, international perspectives, and the history and philosophy of medicine. It is a stimulating and inspiring read for general practitioners and other primary healthcare professionals, undergraduate and postgraduate medical students, healthcare educators, academics, and primary care researchers. Healthcare policy makers and shapers will value its lucid account of complex issues. 'Joachim Sturmberg has written an important book, which I sincerely hope the reformers of our health care system will study carefully. It is also a riveting read. With great erudition and strong arguments, Sturmberg lays out a plan which leads to a goal to which we all aspire - a health care system based on primary care and primary health care which expresses the historic values of medicine and adapts itself to the complexity of modern medicine. A must read for anyone who has the interests of primary care at heart.' - Ian R McWhinney, in the Foreword.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
Medicine
SECTION THREE
The practice of medicine: healing
In particular I believe that cure is rare while the need for care is widespread, and that the pursuit of cure at all costs may restrict the supply of care, but the bias has at least been declared.
Archie Cochrane61
Medical care - who determines what it is, and how is it negotiated between patients and doctors? It is an important question to reflect upon - particularly in light of the philosophical foundations of medicine. Is there a unifying model of health and health care that overcomes the Cartesian reductionism of the past centuries?
Healing is the ultimate goal of medicine. Illness, rather than disease, brings the patient to the doctor. Many illnesses are not associated with a definable disease, and the classical model of curing a disease does not apply to healing of the illness. Healing is the process of coming to terms with ones illness, making sense of that experience in light of ones life circumstances. The relationship between the doctor and the patient creates the therapeutic environment for healing.
The first chapter in this section describes the epidemiology of illness and disease in the community. Illness is common, disease is rare. However the fear of illness and disease has increased markedly over the past 40 years despite the fact that we never experienced better health ever.
The second chapter explores the related but distinctive notions of disease, illness and health. Disease is social in nature, whereas illness and disease is of a personal nature. A dynamic balance model of health is proposed that integrates the somatic, mental, social and sense-making (semiotic) aspects of the health and illness experience, and offers a means to overcome the prevailing Cartesian dualism in health care.
Medicine needs to re-emphasise the need to care. The third chapter argues that medicine must adapt its limited knowledge in the context of a unique understanding of our patients’ needs. Care is based on a personal relationship between the doctor and his patient. This relationship is informed by the diverse knowledge arising from psychoneuroimmunology, technology and evidence-based medicine, all of which affect the process and the outcome of care.
The final chapter examines general practice/family medicine in more detail. The discipline is defined in relationship terms and by its commitment to the person in his community. The personal relationship between doctor and patient enhances the consultation through patient centredness, trust, knowledge about each other and, ultimately, wise clinical decisions. The ongoing relationship provides much-needed stability in a rapidly changing healthcare system, equally benefiting patients and the system.
CHAPTER 10
The epidemiology of illness and disease
Every scientific truth goes through three states: first, people say it conflicts with the Bible; next, they say it has been discovered before. Lastly, they say they always believed it.
Louis Agassiz (1807-1873)
How healthy are the people in our community? Looking at all the media hype about the threats caused by old and emerging diseases we all must be on guard all the time.
How true are these threats really? How much are we influenced by the constant bombardment of threat in our environment? Are we as doctors fuelling the fear of disease, and the vulnerability to succumb to them? Shouldn’t the fact that we survived the evolutionary pressures in pretty good shape be reassuring?
There are two ways of assessing the health state of a community, one by looking at mortality statistics, the other by asking people to report on their health and their responses to experiencing illness.
Mortality statistics have one big irony; we all are going to be one at some stage. The accuracy of mortality statistics is limited by the fact that they are largely compiled on the basis of clinical rather than post-mortem assessments. Mortality data nevertheless are helpful for the planning of health service priorities (see Table 10.1), but they do not tell us anything about the impact of the underlying disease(s) on life. In particular, mortality statistics do not help us in understanding and dealing with a particular patient’s illness experience in the consultation.
TABLE 10.1 Leading causes of death: Australia and Fiji1,2
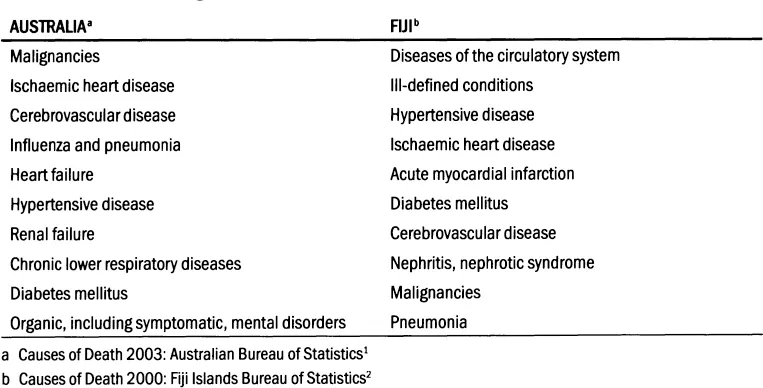
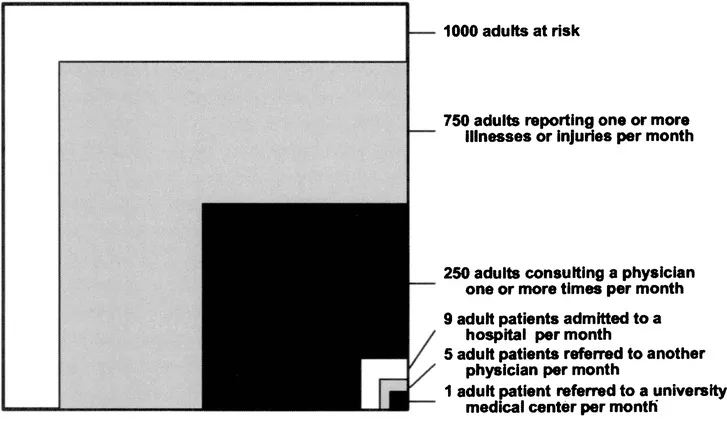
Figure 10.1 Monthly prevalence estimates of illness in the community and the roles of physicians, hospitals, and university medical centres in the provision of medical care. (Reproduced from White K, Williams F and Greenberg B. The ecology of medical care. New England Journal of Medicine. 1961; 265: 885-92,3 with permission from the Massachusetts Medical Society.)
White and colleagues explored the health and illness experience of the community and described a rather bright picture - most members of a community perceive themselves to be healthy and able to cope by themselves with most minor illness symptoms. Only a small percentage of those seeking medical care are subsequently diagnosed with a disease and/or require specialised medical services (seeFigure 10.1).3
Community health and illness has changed little between 1961 and 2001. Larry Green and colleagues reviewed current data, and found that many more patients experience some illness symptoms and that about 30% more people seek care, mostly from complementary and alternative medical care providers.4 These changes may well reflect the impact of the media hype alluded to above. There also has been a shift towards ambulatory/community care reflecting to some extent the needs of an aging population, and to another our greater ability to provide care based on technological advances. However, the number ofpatients requiring hospital care remains unchanged (seeFigure 10.2).
It is rather remarkable how stable the epidemiology of disease has been over these four decades. It is equally remarkable to see that at a time when the population at large has never been healthier, the population also appears to be more afraid than ever of illness and death.5 Figure 10.3 illustrates an analysis of the community’s health-seeking behaviour - two questions of great importance arise: ‘How did the community’s perception of being ill change?’ and ‘How do individuals decide when and whom to consult when perceiving the need for medical care?’.
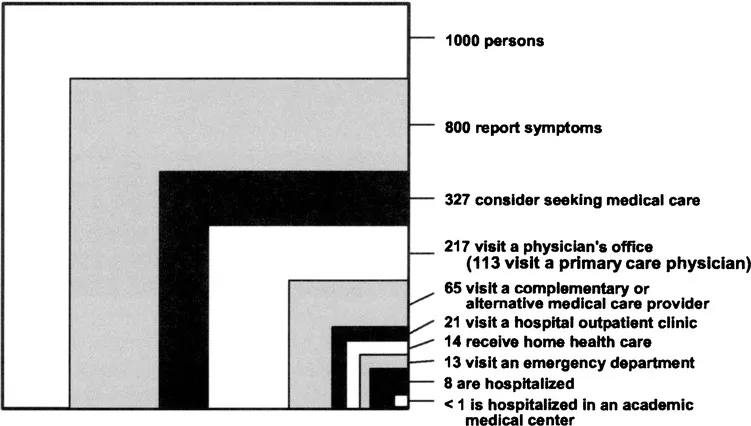
Figure 10.2 Re-analysis of the monthly prevalence of illness in the community and the roles of various sources of health care. (Reproduced form Green L, Fryer G, Yawn B, Lanier D and Dovey S. The ecology of medical care revisited. New England Journal of Medicine. 2001; 344:2021-5,4 with permission from the Massachusetts Medical Society.)
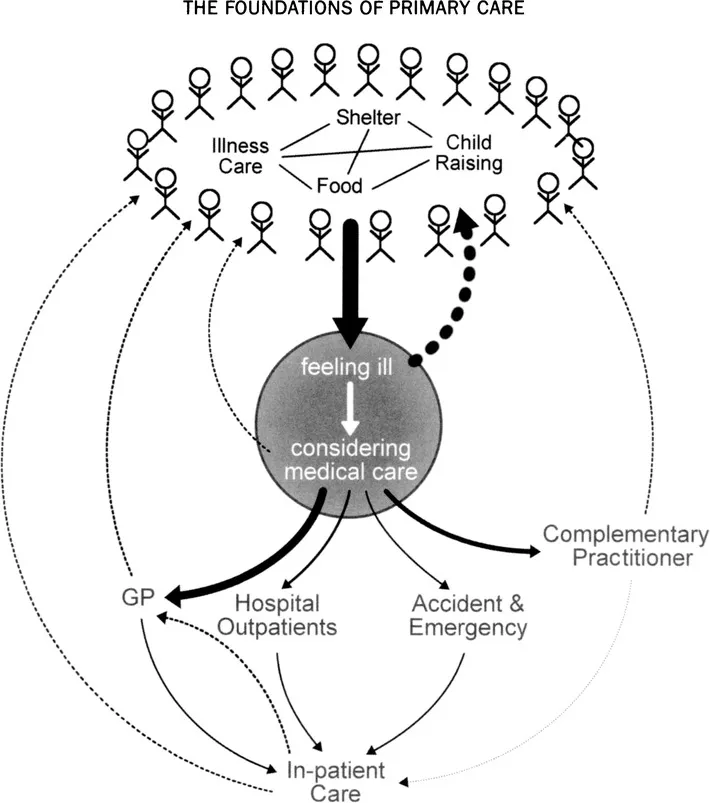
Figure 10.3 Care-seeking in the community: experiencing illness is common, seeking care is much less common.
Summary Points
- Over the past 45 years the illness experience within Western communities has increased significantly; however, the incidence of serious disease has remained stable.
- People never lived a longer and more disability-free life ever; however, they appear to be more fearful of illness and death.
CHAPTER 11
Disease, illness and health
It is more important to know what patient has a disease, than what disease the patient has.
Sir William Osier
Each man has his particular way of being in good health.
Emanuel Kant
The focus of medicine has shifted beyond the question of an art or a science. No one doubts that sciences have improved our understanding of disease; however, patients do not experience diseases, they only experience the consequences of these.6 Every patient is unique, and no two patients share the same illness narrative even if they have the same disease label.
Illness describes a subjective experience; it is the patient’s account about his state of self.7 Disease, in contrast, is the objective state of physical alteration, defined by abnormal measurements...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Dedication Page
- Contents
- Foreword
- Acknowlegements
- Copyright permissions
- Introduction
- Section One Historical perspective of medicine: from shaman to modern physician
- Section Two Philosophical perspective of medicine: search for the meaning of health and illness
- Section Three The practice of medicine: healing
- Section Four The social function of medicine: the interdependence of health in society
- Section Five Medicine in the community: towards primary care
- Appendix: Declaration of Alma-Ata
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Foundations of Primary Care by Joachim P. Sturmberg,James Dearman in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.