![]()
p.1
Chapter 1
Introduction
Environmental health, public health and housing
There is plenty that is good about housing. Many enjoy security in decent housing that provides a health-promoting living environment, and from there are able to add substantially to their wellbeing and quality of life. This is something to which everyone, regardless of their background, should be able to aspire.
The public health and wellbeing agendas have added to this. There has been a renewed focus on population surveillance, needs assessment, and the development of appropriate evidence-based interventions that are able to protect and improve health through housing and allied strategies and interventions. In many areas, this has brought change to how we now intervene in housing, with a renewed focus on health impacts and outcomes across the life course, and most particularly where needs are most acute and negative health effects most keenly felt: for children and older people.
However, there is a flip side to the coin. Since the publication of Environmental Health and Housing in 2001, a substantial amount has changed and increasing numbers are negatively affected by the impact of unsatisfactory housing conditions. The private rented sector has grown substantially, and while many landlords provide decent housing, others do not. The remedy for this is increasingly challenging as the effects of short-term tenancies, high rents and retaliatory eviction take their toll on disempowered and diverse communities of private sector tenants who are trapped in this sector. This is far more about ideology favouring the private housing sector than about health.
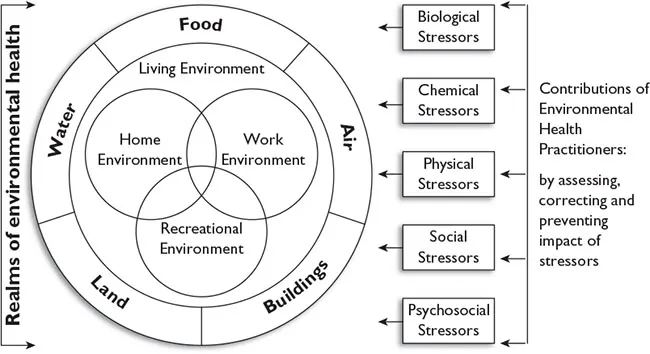
Environmental health policy and practice is both proactive and reactive in creating health-promoting environments (Burke etal., 2002) and active citizenship. It involves a range of knowledge and skills to identify and remove or mitigate a range of environmental stressors that negatively affect physical and mental health (see Figure 1.1). While much environmental health work is based on regulation, new public health arrangements have substantially opened up new partnership opportunities with other stakeholders with an interest in housing, health and safety. This has enabled a far wider remit concerning population health and health inequalities. However, to this end, the most effective evidence-based strategies and interventions must be utilised to protect and improve health, and deliver better health outcomes overall (Stewart, 2013).
p.2
While housing aspects of environmental health are a fundamental part of public health, they are constantly being overlooked in terms of policy development. While social housing is often represented in Joint Strategic Needs Assessment (JSNA), it is not uncommon for housing in the private sector – the majority and growing tenure – to get very little, if any, mention. This has to change. Many in environmental health have been working hard with their partners to explore how a respected and dynamic evidence base could be created and maintained to develop and implement effective evidence-based strategies that deliver increasingly positive and tangible health benefits. We have many tools to help us deliver here, including Health Needs Assessments (HNAs), Health Impact Assessments (HIAs), a range of housing and health resources and toolkits, and housing cost calculators, and these are addressed later in the text.
However, at the same time, those working in environmental health and housing are under increasing pressure around regulation and to meet performance targets, which may or may not have a basis in health promotion, protection or improvement. Often, the focus is on ‘outputs’, such as number of premises inspected, rather than ‘outcomes’, such as the number of people whose health has improved due to better housing.
In addition, an ageing population places substantial new demands on housing. Most people wish to remain in their own housing for as long as possible, but when this is no longer possible, due to frailty or degenerative disease, such as dementia, many may need to move into purpose-built or adapted housing to meet their ongoing, changing needs. While purpose-built ‘older people’ developments may be part of the solution, support needs to be given to assistance at home, suitable types of transition accommodation (bungalows, for example) and ensuring integration, not segregation, of older people.
p.3
People, of course, do not just live in formal ‘housing’, and we will look at some definitions later on, as well as concepts in tenure and homelessness. Some have had to find alternative living arrangements, either through culture and heritage, or complete lack of choice and affordability in the housing market. For example, some people live in caravans or mobile homes, and there is a complex array of laws addressing conditions, licensing requirements and even issues to consider such as trespassing in these cases. Some people build their own accommodation ‘informally’, or live in places now known as ‘beds in sheds’, and suffer the planning consequences. Others have nowhere at all to live and are deemed ‘rough sleepers’. Some find themselves with no recourse to public funds (NRPF).
Environmental health largely focuses on a regulatory approach that is useful and important, with a range of civil and criminal actions. This, however, is only part of the picture. A far wider engagement with public health is essential to consider the range of health inequalities and determinants in order to more sustainably improve health outcomes.
Despite multiple and complex challenges, many organisations work to support those living in poor housing across tenures. While this book does touch on all tenures, there is a major focus on private sector housing – owner-occupation – and most particularly the private rented sector, where some of the poorest housing conditions are found and where many vulnerable people live, often through lack of choice in the housing market. A whole chapter is therefore dedicated to regulation of this sector, and some of the unique factors found there.
We refer in this book largely to Environmental Health Practitioners (EHPs), who are generally the professional front-line group addressing housing conditions. In this definition, we are also including others working in this sector who – while not EHPs by qualification – are skilled in assessing housing deficiencies and what to do about them both in practice and the processes required. Where we say EHP in this book, we therefore also refer to the numerous others involved: housing surveyors, housing technicians and technical officers.
What we also need to say here is what we do not include in this book. This is a book about England and Wales, where the main Housing Acts are similar, although regulations and national surveys are not. We are unfortunately unable to cover Northern Ireland, where certificates of fitness are issued, or Scotland, which applies the tolerable housing standard. Each nation also has its own public health agenda. We would also say that while the links around housing, health and safety are similar across tenures, this book focuses largely on the private housing sector together with the legislation and public health strategies and interventions to help tackle poor and inappropriate housing conditions.
p.4
We close the introduction with this thought, proffered by David Seedhouse (2001: 134), who asks us:
We extend this idea to health and housing, asking in this book what housing is for. Is it to be a commercial, market asset, or is to be viewed as a primary determinant of health to help ensure that everyone has a better life?
For us, it is the latter. We hope that readers of this book will think so too, and will do what they can about it.
Synopsis of the book
• Chapter 2 Why environmental health, public health and housing?
• Chapter 3 Gathering evidence
• Chapter 4 Legislation for healthier and safer housing
• Chapter 5 Working more effectively together
• Chapter 6 Conclusions
![]()
p.5
Chapter 2
Why environmental health, public health and housing?
This chapter looks at:
2.1 A very brief history of housing
2.2 Housing stock, conditions and need
2.3 Housing and inequality: Marmot and the social determinants of health
2.4 Living on the margins: from (statutory) homelessness to rough sleeping
2.5 Housing as home
2.6 Home safety and home accidents
2.7 Fire safety in dwellings
2.8 Fuel poverty and cold, damp homes
2.9 (Over)crowding and space standards
2.10 Tuberculosis (TB) and housing
2.11 Gypsies and travellers
2.12 Mental health and green and blue spaces
2.13 Loneliness, isolation and the potential of social capital
2.1 A very brief history of housing
The massive influx from country to town during the Industrial Revolution put huge pressure on urban areas. Edwin Chadwick made the link between health and housing in his self-funded Sanitary Conditions of the Labouring Population of Great Britain in 1842. He painted a desperate picture of overcrowded, damp, unventilated houses lacking adequate drainage and proper water supplies, leading to low life expectancy and disease (see also Stewart, 2017).
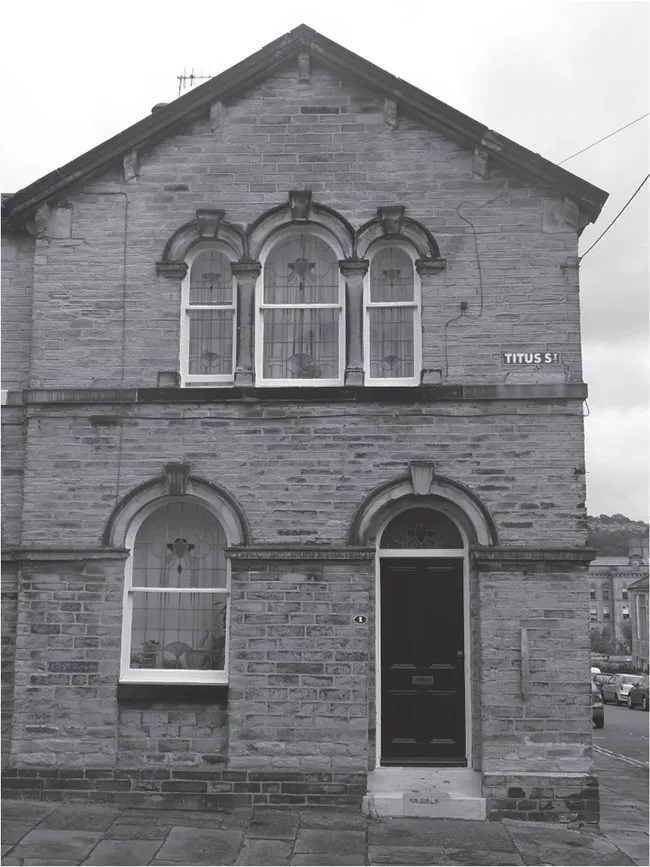
At this time, it was largely left to factory owners and philanthropists to provide and manage working-class housing. Titus Salt provided a workers village called Saltaire in 1853 (see Figure 2.1), and later other developments followed, including Port Sunlight and George Cadbury’s Bournville, which gave better living conditions but were also linked with paternalist management (Lynch and Dhesi, 2017) (see Figures 2.2 and 2.3). Octavia Hill established the first ‘social housing’ scheme around 1865. There was also interest in promoting social change (such as the social reforms driven forward by the Rowntree family) and a drive to understand the nature and extent of poverty, notably highlighted by Charles Booth (Wise, 2009; Clough, 2017).
p.6
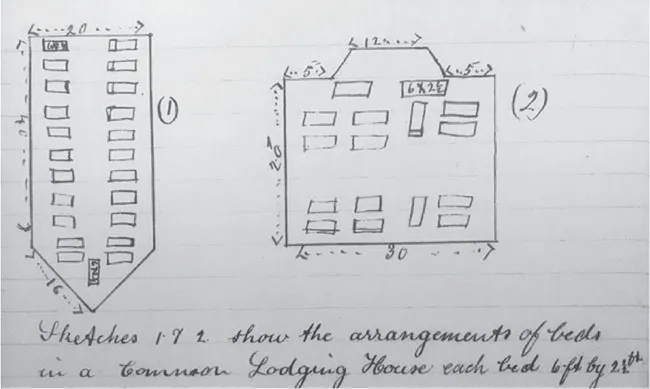
Alongside housing reform in the 1850s came regulations to tackle conditions in common lodging houses, but no additional resources were made available for local authorities to tackle the issues. Original extracts from a sanitary inspector’s notebook are shown in Figure 2.4. Continued pressure for legal improvements gained momentum, and new legislation continued to enable local authorities to deal with individual insanitary houses, although not yet areas of bad housing, and with very little resources for building new housing.
p.7
p.8
The Housing of the Working Classes Act 1890 drew together the miscellaneous ad hoc housing schemes in an attempt to consolidate best policy and encourage housing where none currently existed. The Act provided for dealing with unhealthy areas, improvement schemes and unfit dwelling houses, and gave powers to provide lodging houses. This provided the administrative framework for later housing measures. However, it came with no additional funding, and local authorities were expected to raise the money themselves. The Housing and Town Planning Act 1909 gave local authorities powers to control development and introduced some controls, such as prohibiting back-to-back houses, and recognised the role of building societies in housing. Prior to the First World War, less than 1 per cent of housing stock had been provided by municipal and philanthropic activity, and major regional variations remained. The Boundary Estate (see Figure 2.5) was a notable exception, being a large local authority social housing scheme built despite some major concerns about resident displacement and rental costs (Wise, 2009). It still provides attractive Arts and Crafts-inspired housing in London.
Into the twentieth century
p.9