![]()
PART I
Developmental language disorder in context
![]()
Introduction
James Law
This book is about the management of children and young people with developmental language disorders (DLD). DLD is a relatively common condition affecting children and young people. The latest figures suggest that 9 per cent of children experience it at school entry. DLD occurs when the child’s language skills are judged to be significantly delayed relative to those of children of the same age. This judgement is usually made by means of a combination of formal assessment, observations of linguistic performance and professional judgement.
DLD is often described as being either primary or secondary. Primary DLD occurs when the child’s difficulty is principally with language (although there may be other comorbid conditions such a behavioural disorders, conductive hearing loss, etc.) Secondary DLD occurs when the child’s difficulty is associated with a broader condition (e.g. cerebral palsy, autism, sensori-neural deafness, etc.). The main focus of this text is the child with primary DLD. A recent multinational and multidisciplinary Delphi consensus study of practitioners in the English-speaking world, “Criteria and Terminology Applied to Language Impairments: Synthesising the Evidence” (CATALISE), recommended that the term language disorder be used for children whose language difficulties are likely to persist and/or who experience “functional limitations” such as poor educational attainment, limited everyday communication, social relationships and quality of life as they move into the school years (Bishop et al., 2016, 2017) with the additional designation of developmental language disorder, for those children meeting these criteria, and whose language disorder is not associated with certain known biomedical aetiologies. The latter thus refers to primary language disorder. Central to this is the services that are available for these children and how they are organized, delivered and evaluated. It is important to comment than when the network, which is the topic of this book, was initiated the term “language impairment” (LI) was used. In accordance with the consensus statement we have opted to use the term DLD throughout this book.
Sometimes there is confusion between children who seem to have difficulties learning more than one language and experience difficulties as they shift between them, and those who have a difficulty acquiring their first language. Although it is recognized that the two sometimes overlap, the main focus of this book is the child with difficulties learning their first language. DLD does not occur because a child uses more than one language. A bilingual or multilingual child may experience DLD but this would normally be in each of the languages concerned. The emphasis is also on oral language rather than any alternative or augmentative language systems.
This book addresses the way that the needs of the child with developmental language disorders are met across Europe. It grew out of the work of COST Action 1406 entitled Enhancing Children’s Oral Language Skills Across Europe and Beyond: A Collaboration Focusing on Interventions for Children with Difficulties Learning Their First Language. This was an EU-funded research network that ran between 2015 and 2019 and incorporated representation from 36 countries, the majority of which were members of the European Union but that included some “near-neighbour” countries such as Lebanon and Albania and some international partners such as South Africa. As part of the work of this group a survey of practice related to children with developmental language disorders was carried out in 2017.
The book is organized in two halves. In the first we consider the context of evidence-based practice in this field, how the survey works and the main findings from the survey itself, looking at the theoretical underpinnings of intervention, the way that services are arranged and the cultural context in which they are delivered. In the second we asked members of the network and their colleagues to write short vignettes about the history of the way that DLD has been identified and treated in their country and their priorities for the future development of research, on the one hand, and services, on the other.
It needs to be said that clearly the development, translation, circulation and analysis of the practitioner survey was an enormous undertaking involving many people in every country involved in the project. We acknowledge the amount of work involved and thank them for the time they put into it. COST Actions may fund the networking but they do not fund the research. We would also like to thank our administrator, Nikki Hawley at Newcastle University, for helping to coordinate this complex undertaking. We also need to acknowledge the additional work that contributors put in by writing the country vignettes and I would like to pay tribute to their endeavour in contributing to what is the first book of its kind to represent the European tradition in the study of developmental language disorders and speech and language therapy more generally.
References
Bishop D.V.M., Snowling, M.J., Thompson, P.A., Greenhalgh, T. and the CATALISE-2 consortium. (2016). CATALISE: A multinational and multidisciplinary Delphi consensus study of problems with language development. Phase 2. Terminology. PeerJ Preprints, 4: e2484v1. https://doi.org/10.7287/peerj.preprints.2484v1.
Bishop, D.V.M., Snowling, M.J., Thompson, P.A., Greenhalgh, T. and the CATALISE Consortium. (2017). CATALISE: A multinational and multidisciplinary Delphi consensus study identifying language impairments in children. PLOS One, 11(7). http://dx.doi.org/10.1371/journal.pone.0158753.
![]()
Evidence-based practice and its application to developmental language disorders James Law | 1 |
Introduction
In this chapter we look at the culture of “evidence-based practice” that has become such a key element of the underlying rationale for the management of health care in developed, and indeed developing, countries. Historically the principles underpinning evidence-based practice apply across all branches of health care and over the past 20 years great steps have been taken in the treatment of children with developmental language disorder (DLD) and in the field of speech and language science more generally to use evidence to inform practice. Here we look at what we understand by evidence-based practice and its component parts and ask how easy it really is to integrate such disparate sources of information. We then turn to the broader educational context in which practices, whether evidence-based or otherwise, are implemented in educational policy and ask what role overarching professional bodies have in co-ordinating, directing or simply nudging practice across Europe. The detail of the survey that is the focus of this book is described in more detail in Chapter 2 and the primary results in Chapters 3, 4 and 5.
The culture of evidence-based practice
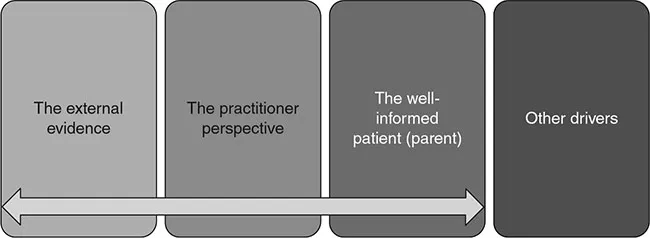
The concept of scientific-based medicine has a long history that has been well rehearsed. Two key figures stand out. The first is James Lind, who was an eighteenth-century Scottish physician and a pioneer of naval hygiene in the Royal Navy. By conducting one of the first ever clinical trials, he developed the theory that citrus fruits prevented scurvy aboard naval ships. Using this empirical approach he argued for the health benefits of better ventilation, the improved cleanliness of sailors’ bodies, clothing and bedding, and below-deck fumigation with sulphur and arsenic. He also proposed that fresh water could be obtained by distilling seawater. Archie Cochrane was a Scottish doctor noted for his book Effectiveness and Efficiency: Random Reflections on Health Services (Cochrane, 1972). This book advocated the use of randomized control trials to make medicine more effective and efficient. But there are many who have advocated the integration of external robust evidence with clinical judgement. This is summarized by Dollaghan (2007, p. 2) as “the conscientious, explicit, and judicious integration” of the following:
1. The best available external evidence from systematic research.
2. The best available evidence internal to clinical practice.
3. The best available evidence concerning the preferences of a fully informed patient.
And is commonly conceived of as a series of pillars or legs of a stool. On the whole these pillars are considered to be discrete, although there is clearly a need to integrate them at some level (Law et al., 2015). In addition, there is often a fourth pillar that we have captured here as “other drivers” corresponding to the context in which an intervention is delivered. We look at each of these components below (Figure 1.1).
External evidence
Previous reviews have largely been narrative in nature and thus prone to bias (Goldstein and Hockenburger, 1991; Enderby and Emerson, 1996; Law, 1997; McLean and Woods Cripe, 1997; Gallagher, 1998; Guralnick, 1988; Leonard, 1998; Olswang, 1998; McCauley and Fey, 2006). Two systematic reviews (Nye et al., 1987; Law et al., 1998) were published prior to the publication of the first Cochrane Review in the field (Law et al., 2003). A number have followed it covering specific subpopulations or practice contexts, for example, related to developmental screening (Nelson et al., 2006), interventions for preschool children only (Schooling et al., 2010), educational contexts (Cirrin and Gillam, 2008), receptive language impairments (Boyle et al., 2010), parent–child interaction (Roberts and Kaiser, 2011), grammatical development (Ebbels, 2013), computerized interventions (Strong et al., 2011), late talkers (Cable and Domsch, 2010), language/literacy (Reese et al., 2010), and vocabulary learning in typically developing children (Marulis and Neuman, 2010).
The original Cochrane Review related to DLD triggered a number of discussions about whether the approach employed in the review was the most effective, given the constraints associated with the subject domain and effectively captured in the Medical Research Council (MRC) guidelines (Craig et al., 2008; see also Pring, 2004; Johnston, 2005; Law et al., 2005; Garrett and Thomas, 2006; Marshall et al. 2011). While clinical guidelines to direct practice in speech and language therapy (SLT) do exist, the gap between them and the external evidence often remains a challenge (Autti-Ramo et al., 2014) and there is little in the way of specific guidance on what type of intervention to offer children with DLD.
Systematic reviews are part of the solution but they need to be seen within the context of practitioner expertise (Centre for Community Child Health, 2011; Marshall et al., 2011). We know less about how to integrate the views of practitioners and parents and how effective we are in eliciting evidence-informed patient choice. Although there has been some progress in the field of shared decision-making (Elwyn et al., 2012), the emphasis is commonly on the technical elements of systematic reviewing and the other elements often appear to be the poor relations in the process. Barriers to implementation are legion and practitioners tend to use them to reinforce existing practice rather than question it. In part this reflects the fact that such interventions are inherently complex in their delivery, organizational levels and the degree of flexibility of intervention permitted. Increasingly, Sackett’s original definition is being revisited and reinterpreted to reflect a growing awareness of the need to mesh research with current practice and service user perception (Sackett et al. 1996). Key to understanding this process is to obtain a better description about what practitioners actually do with children with DLD and this is the focus of the chapters in this volume.
Underpinning the use of external evidence is a common assumption about the inherent value of the randomized controlled trial (RCT). Much has been written about this particular approach to evaluation and whether it should be considered the benchmark for the evaluation of health care, education, social work, etc. Although there are some contexts in which more complex designs are necessary, for example testing the feasibility of a given intervention with potential participants or capturing routine practice, the case for the use of RCTs in health care generally is now pretty unassailable. The same is much less clear in education and social work where contextual variables are often considered to play such an important part. There are some organizations, such as the UK’s Education Endowment Foundation, which aims to drive forward the evaluation of educational interventions using this particular approach to intervention but the effects of such behavioural and pedagogical interventions are often modest, commonly with effects sizes of 0.2 in quantitative terms, and many practitioners do not f...