TIME'S NOW for Women Healthcare Leaders: A Guide for the Journey
Women comprise over 80 percent of healthcare frontline employees, but they often hit the proverbial glass ceiling. Only 30 percent of healthcare C-suite Executives and less than 15% of CEOs are women. Moreover, while 51 percent of medical students are women, only 16 percent of the Department Chairs and Deans are women. Clearly, women are facing barriers to achieving their potential, limiting their ability to add their unique talents and skills to the tables of leadership. The author provides extensive detail on these barriers and approaches to their solutions. This is a practical "how-to" book that will help women in healthcare envision their ability to contribute and inspire them to lead. The author sees this as not only helping women, but also facilitating solving healthcare's myriad problems, improving health and benefitting society.
***
This book is a must-read primer for women seeking leadership. It is practical, thought provoking, and carefully researched, addressing why women's leadership is important and how women can be better leaders. Gabow's approach capitalizes on interviews with strong women leaders. She uses the notions she learned from the interviews coupled with research from the literature to create an easy-to-read, motivating, and challenging book for women and men!
Nancy Agee President and CEO Carilion Clinic Past Chair American Hospital Association
TIME'S NOW for Women Healthcare Leaders is filled with powerful examples of how women have overcome multiple obstacles and prevailed on their leadership journeys. It is a MUST read for women and men about the obstacles to be overcome, potholes to avoid, and the shout outs to be given to women who every minute, every hour, every day are committed to human caring. It has captured the heart and spirits of women from diverse backgrounds who have and continue to demonstrate their commitment to making society a better place for all!
Linda Burnes Bolton, DrPH, RN, FAAN Senior Vice President and System Chief Equity Officer Cedars Sinai Health System
This highly engaging book addresses the relative dearth of women leaders in healthcare through thoughtful assessment of how leaders' values and actions can improve healthcare within healthcare organizations and systems. Dr. Gabow, an exceptional leader whose relentless passion for excellence for patients served by Denver Health earned her national renown, combines insightful observations from her own path with current statistics about women in medicine, experiences of other successful women leaders, and mentoring skills to offer wise counsel to all current and future leaders. The thoughtful distillation of practical wisdom offered here make this book a unique contribution and highly relevant to healthcare in America today.
Carolyn Clancy, M.D. Past Director, Agency for Healthcare Research and Quality
This insightful book is full of personal stories, honest reflections, and data-driven guidance from and about women leaders. It serves as a wonderful resource for those motivated to advance diverse and inclusive organizations.
Karen DeSalvo, M.D., MPH Chief Health Officer, Google Health Past Acting Assistant Secretary for Health, US HHS National Coordinator for Health Information Technology, US HHS
Frequently asked questions
Simply head over to the account section in settings and click on “Cancel Subscription” - it’s as simple as that. After you cancel, your membership will stay active for the remainder of the time you’ve paid for. Learn more here.
At the moment all of our mobile-responsive ePub books are available to download via the app. Most of our PDFs are also available to download and we're working on making the final remaining ones downloadable now. Learn more here.
Both plans give you full access to the library and all of Perlego’s features. The only differences are the price and subscription period: With the annual plan you’ll save around 30% compared to 12 months on the monthly plan.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 1000+ topics, we’ve got you covered! Learn more here.
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more here.
Yes, you can access TIME'S NOW for Women Healthcare Leaders by Patricia A. Gabow in PDF and/or ePUB format, as well as other popular books in Business & Women in Business. We have over one million books available in our catalogue for you to explore.
“What changes when a woman leads business—Everything.”
Goldman Sachs Ad New York Times October 7, 2018
There are three short, straight-forward answers to the question, “Why should women lead?” The first is that fairness demands women have equal representation in healthcare leadership. The second is that in not achieving gender equality in healthcare leadership we are failing to utilize all the available talent. The third is that healthcare has myriad problems and women leaders can bring a new and needed perspective to the solutions. These answers are based on a series of general and healthcare-specific facts:
Women are 50.8 percent of the United States population.
Women constitute 47 percent of the American workforce (74.6 million civilian workers).
Women’s presence in the workforce accounts for 25 percent of GDP.
Women make up 75 to 80 percent of the healthcare workforce but less than 15 percent of the top leadership positions.
Women make 80 percent of the healthcare buying and use decisions.
Women are 75 percent of the family caregivers.
Women bring unique perspectives and skills to leadership.
If the Goldman Sachs’ declaration above is true, and I believe it is, then women must answer the call to become healthcare leaders. Moreover, if women constitute the majority of the healthcare workforce, why should men primarily develop and oversee policies, conditions, and goals in the system? Women need to be equally represented among healthcare leaders not solely, or even most importantly, for their own benefit, but for what they will bring to health and healthcare. If, as women, we succeed in achieving fair and equal leadership representation throughout healthcare, but our presence does not drive major transformation, the full promise of women’s healthcare leadership will not have been achieved.
Men have almost exclusively led all the components of our society that have shaped American healthcare: physicians, health systems, insurance companies, pharmaceutical and device industries, and government. This is not to say that male leaders are the cause of our healthcare system’s problems. But it is to say that we need a different outcome and if we are to achieve that outcome, we need different voices at the table—women and men, people of color and white individuals, and the young and old.
American Healthcare
While American healthcare has achieved amazing breakthroughs in some areas, it is failing in many aspects and is not delivering population health, both objectively, and in comparison to other developed countries. If women are to play a pivotal role in the solutions, we must clearly see the failures before we can address them. We cannot sing from the old song sheet that America has the best healthcare system in the world. We need to be clear that although the system is exceptionally good in some ways, it is exceptionally bad in others. We must preserve and build on what is good and minimize or eliminate what is bad.
Thought Exercise
What do you see as the major issues in our healthcare system? How do we compare in outcomes with other high-income countries (HIC)?
In assessing the performance of our healthcare system, we need to look at how American healthcare performs in the areas of cost, coverage, access, quality, and disparity/equity. We are currently spending almost 18 percent of nation’s GDP, or $3.5 trillion on healthcare—twice as much as other high-income countries and over the years our costs have risen faster than in any other HIC (National Health Expenditure Data, 2018; Anderson et al., 2019).
Given the complexity of American healthcare, it is not surprising that the causes of this exaggerated healthcare expenditure are myriad:
Prices
Salaries
Care fragmentation
Administrative complexity
Overuse and misuse of therapies
Waste
When asked why American healthcare is so expensive, the well-known health economist, Uwe Reinhardt, famously declared, “It’s the prices, stupid” (Anderson et al., 2003). This central role of prices has recently been confirmed (Papanicolas et al., 2018; Anderson et al., 2019). This work underscores the major contributions of products, including pharmaceuticals, procedures, and people to our sky-high costs. The annual per capita cost of pharmaceuticals in the United States is $1443 compared to a mean of $749 in other HIC (Papanicolas et al., 2018)—$700 per person creates quite a stack of money at the end of the year! This price differential becomes shocking for some high-cost drugs. For example, the average price of Humira in the United States is 96 percent higher than in the United Kingdom (Kamal and Cox, 2018). We have higher costs of high-margin, high-volume procedures. For example, the average cost of a total knee replacement is over $28,000 in the United States and can reach more than $60,000 in some healthcare systems compared to about $18,000 in the United Kingdom (Millman, 2015; Kamal and Cox, 2018). No wonder healthcare tourism has emerged.
We pay more for components of the American healthcare workforce than do other HIC. Physicians, both primary care doctors and specialists, earn almost double that of other HIC. These wages are higher even after correcting for purchasing power and for the average medical school debt of American physicians (Papanicolas et al., 2018). Although there is variability in nurse salaries, hospital-based nurses earn almost $20,000 per year more in the United States than in other HIC (Anderson et al, 2019). The salary differential is more surprising for health system administrators. The highest hospital administrator’s yearly earnings in the United Kingdom in 2015 was a record £340,000, about $430,000 in United States dollars (Donnelly, 2016). The four highest salaries for healthcare system administrators in the United States ranged from $10 million for the CEO of Kaiser Permanente to over $17 million for the CEO of HCA, and 17 hospital administrators in the United States earned over $5 million per year (Knowles, 2018).
The care of patients is often fragmented due to lack of a primary care physician, use of emergency departments for care amenable to ambulatory care, and inadequate communication between providers and systems of care. The fragmentation and complexity are compounded by myriad insurance coverages, all with different benefits and rules. Even at the federal level, there is coverage via Medicare (with its multiple alphabet components), Medicaid (with a version for every state and territory), the Child Health Plan (with state variations), the Veterans Health Administration, the military services health system, and the Federal Employees Health-Benefits Plan. If this wasn’t enough, there are hundreds of health insurance companies. Because of the fragmentation and complexity, administrative costs in the United States are about 8 percent of total healthcare expenses compared to 3 percent in other HIC (Papanicolas et al., 2018). These administrative complexities have human costs in burdening providers and patients as well as financial costs to the system.
Despite spending a great deal more than other HIC, unlike these other countries, we do not provide health insurance coverage for everyone. In 2013 there were 44 million Americans who were uninsured (Kaiser Family Foundation, 2018). By 2016, with the implementation of the Affordable Care Act (ACA), that number had fallen to 26 million—much better, but still not zero. However, by 2017 the number of uninsured had increased by 700,000 people (Kaiser Family Foundation, 2018). These numbers will likely continue to grow as the federal government and many states seek to significantly alter the ACA and Medicaid coverage. With the advent of high-deductible plans, even the insured are often substantially underinsured.
In America insurance matters. In 2017, the uninsured were four times more likely than those with Medicaid or private insurance to lack a usual source of care, and these patients were much more likely to postpone care, go without care, or not fill a prescription because of cost—hardly a path to well-being (Kaiser Family Foundation, 2018). Those of us who take care of patients understand that as important as health insurance is as a ticket to healthcare, it does not guarantee access. Recent access problems with long waiting times for care within the Veterans Health Administration dramatically underscored this reality. Access, especially to specialty care and dental care, is also a problem for Medicaid patients, as some physicians and health systems either limit their numbers or do not take them.
Even when individuals get access to care, they do not always receive the appropriate preventive care or care that is indicated. In fact, 10 to 30 percent of the care they do receive is either not indicated or harmful (McGlynn et al., 2003). In 2018 the Medicare Payment and Advisory Commission (MedPAC) noted, “there is substantial use of low value care—the provision of a service that has little or no clinical benefit or care in which the risk of harm from the service outweighs its potential benefit” (Medicare Payment and Advisory Commission, 2018). This low value care cost Medicare as much as $6.5 million in 2014 (Medicare Payment and Advisory Commission, 2018).
You would think that since we spend twice as much as other HIC on healthcare, the outcomes for Americans would be significantly better than that in these other countries. Sadly, this is not the case. One commonly used measure of care is life expectancy, as most of us desire a long life, and it is an unambiguous endpoint with reliable data. The United States has the lowest life expectancy of all HIC— more than three years less on average (Gonzales et al., 2019). That might not seem like much, unless it is you or your family. Not only is our life expectancy lower; it has fallen for three successive years for the first time since 1915–1918, when the First World War and the Spanish flu were taking their toll (Dyer, 2018). This shortened life expectancy starts from birth. The United States has the highest infant mortality of all HIC.
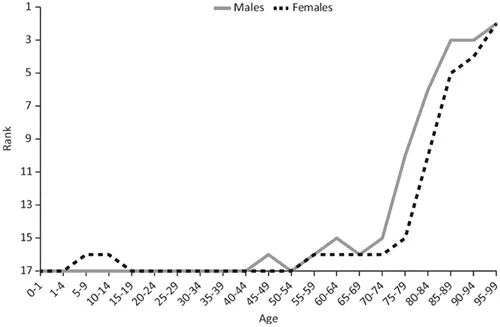
There are several ways to look at this decreased life expectancy, which are surprising, if not shocking. One way is to compare life expectancy against healthcare spending. For almost all countries, spending more on healthcare increases life expectancy—not so for the United States. We are an outlier, spending more and getting less (OECD, 2018). Another way to look at this is to see where the United States ranks in life expectancy across all ages compared to 17 other HIC. Given that it is often stated, “We have the best healthcare system in the world,” one might expect that we would be number one or at least two or three across the board—far from it. We never rank above 15th out of 17 countries until age 75, and we achieve the highest life expectancy among 95-year-olds, when most of us are dead (Figure 1.1) (Institute of Medicine and National Research Council, 2013)! In a range of other quality measures, we underperform compared to other HIC, including having a higher mortality for conditions amenable to healthcare.
Figure 1.1 Ranking of U.S. mortality rates by age group among 17 peer countries. Number 1 is the top ranking with the lowest death rate and number 17 is the lowest ranking with the highest death rate. (Source: Institute of Medicine and National Research Council. 2013. U.S. Health in International Perspective: Shorter Lives, Poorer Health. https://doi.org/10.17226/13497. Reproduced with permission from the National Academy of Sciences, Courtesy of the National Academic Press, Washington, D.C.)
Within America, there is considerable variability in coverage, access, and outcome by race, socioeconomic group, and geography. African Americans, Native Americans/Alaskan Natives, and Hispanics are less likely to have insurance coverage, and they attain lower health status and poorer outcomes. African Americans fared worse than whites in 24 of 29 measures, Native Americans/Alaskan natives on 20 of 29 measures and Hispanics on 11 of 29 measures (Artiga et al., 2016). There is marked geographic variability across the states, within counties in states, and even within a single city. Generally, health is poorer in the southeastern part of the United States than the rest of the country (Radley et al., 2018). Health outcomes vary across counties in every state (County Health Rankings and Roadmap, 2019). The variation within ...
Table of contents
Cover
Endorsements
Half-Title
Title
Copyright
Dedication
Contents
Foreword
Acknowledgments
Author
Introduction
1 Why Should Women Lead?
2 Lay of the Land
3 Obstacles and Opportunities
4 First Things First
5 You Can’t Parachute into Leadership
6 Now You Are a Leader
7 Even Leaders Have a Boss
8 Making the Trains Run on Time and Laying New Tracks