- 192 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
The control of E.coli 0157 is at the heart of the environmental health practitioner's professional agenda. This book is aimed at health professionals who need to be fully informed about the sources and effects of the organism in order to provide advice and enforce legislation at local level as well as providing non specialist professionals with a p
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Subtopic
Architecture Methods & MaterialsChapter 1: Overview
Escherichia Coli (E.Coli) Bacteria Are Common Commensals Of The Gastrointestinal Tract Of Humans And Animals. There Are Many Different Strains Of E.ColiAnd Only A Few Cause Disease. This Book Is About Those Strains Of E.ColiWhich Produce Toxins Known As Vero Cytotoxins Which Damage The Intestinal Tract, And Which In Some People Cause Serious Kidney Failure.
Several serotypes of E.coli can produce these toxins and they are collectively known as VTEC. However, in the UK the principal cause of VTEC disease is E.coli O157. There is no specific treatment for this: antibiotic treatments have been used but there is no indication from several studies that they reduce the length of illness, therefore prevention is particularly important. In comparison with other pathogens which cause diarrhoea in the UK (Figure 1.2) the incidence of VTEC O157 is very low. On average, an Environmental Health Officer (EHO) is likely to investigate less than one sporadic case per year and is very unlikely to ever have to investigate an outbreak. He or she is therefore unlikely to be an expert on the investigation and control of the disease. However, when cases do occur, the EHO plays a key role in investigating and preventing further spread. The following text provides easily accessible, practical information.
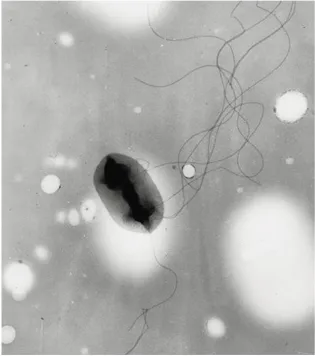
Figure 1.1 E.coli bacteria
E.colis which cause disease
Typing of E.coli is based on the identification of lipopolysaccharide capsular antigens, the somatic ‘O’ antigens and the flagellar H antigens. VTEC O157 possesses ‘O’ antigens 157 an ‘H’ antigen 7. Together they constitute the serotype O157:H7. E.coliwhich caused diarrhoea can also be categorised on the basis of the mechanisms by which they cause the diarrhoea (Table 1.1).
Enteropathogenic (EPEC): The first of these was recognised in 1940. This infection has been associated with outbreaks of diarrhoea in young children. Illness is caused by the bacteria adhering to the intestinal wall.
Table 1.1 Categories of diarrhoeagenic E.coli
Enterotoxigenic (ETEC): This category came to prominence in the late 1960s and was associated with infant diarrhoea in developing countries as well as traveller’s diarrhoea. The acute watery diarrhoea is produced by heat stable or heat label toxins.
Enteroinvasive (EIEC): Enteroinvasive E.coli were first described in 1971 and are very closely related to Shigella bacteria causing dysentery type illness in humans by the invasion of the gut epithelial cells.
Enterohaemorrhagic (EHEC): The emergence of VTEC in the early 1980s led to the recognition of enterohaemorrhagic E.coli associated with haemorrhagic colitis and haemolytic uraemic syndrome. Other EHEC have been recognised which are all vero cytotoxin producing. Vero cytotoxin is a toxin which destroys vero cells, a particular laboratory cell line, and also affects the cells lining the gastrointestinal tract and the kidneys. Further information on how VTEC cause disease is given later in this chapter.
Enteroaggregative (EaggEC): More recently enteroaggregative E.coli have been associated with persistent diarrhoea in people in developing countries. They have been isolated in some patients in the UK. A further group, called diffusely adherent E.coli, has been identified and has caused persistent childhood diarrhoea in Bangladesh.
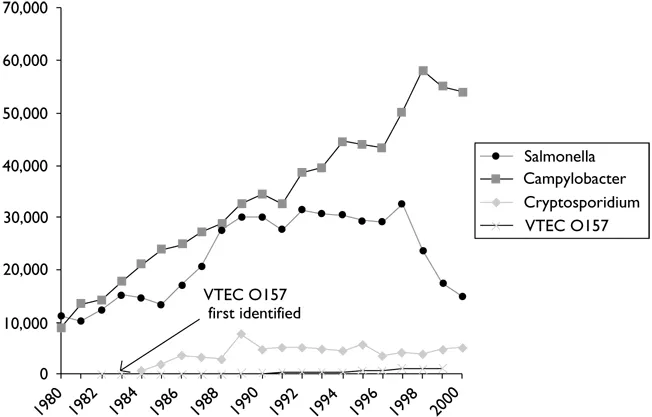
Figure 1.2 Incidence of food poisoning in England and Wales, 1980–2000
Source:Public Health Laboratory Service data (www.phls.co.uk)
The mechanisms of disease in all the strains described above depend upon genetic information, contained often on plasmids or bacteriophages or on chromosomes whose products are regulated by plasmid-encoded genes. The consequence of this is that the virulence traits can be transferred from one serotype of E.coli to another if they exchange genetic information on plasmids or bacteria phages. This frequently occurs in bacterial populations.
The emergence of VTEC O157
VTEC emerged in the 1980s in the United States and has since been recognised worldwide as a major cause of both self-limiting diarrhoea and more serious long-term illness, in particular, haemolytic uraemic syndrome. The way in which VTEC was recognised as a new public health problem is important to note because it teaches several epidemiological and environmental health lessons.
Two outbreaks occurred in the United States in Oregon and in Michigan in February and June 1992. A total of 47 cases were identified in people with a gastrointestinal illness which had some unusual characteristics. The main symptoms were severe colicky abdominal pain so serious that patients sometimes were admitted to hospital under the surgeons for suspected perforated bowel. They also had diarrhoea which was heavily blood stained. Normal faecal examinations did not reveal the expected bacterial infections such as Salmonella, Campylobacter or Shigella, but detailed laboratory investigations carried out at the Centers for Disease Control, Atlanta, identified an E.coli strain O157 from half of all the faeces specimens. Samples of faeces from well people were also examined and none of those produced this strain of E.coli Epidemiological investigations linked the cases to consumption of beefburgers at a single chain of fast food restaurants. Microbiological examination of the frozen raw beef that was used in these restaurants in Michigan identified the same serogroup of E.coli O157. Sophisticated discrimination of the strain of the organism confirmed that the isolate from the raw meat and from clinical (patient) samples were indistinguishable (Riley et al. 1983)
These investigations are excellent examples of the power of epidemiological studies. They were the first outbreaks in which the clinical presentation called haemorrhagic colitis was recognised, and they identified beefburgers from fast food chains as the major vehicle of infection. Since this recognition many other similar outbreaks have been identified across the world.
The environmental health investigations were important to note. The method of contamination of the food from these fast food restaurants was carefully determined. The patty of beef recovered from the supply chain which produced the E.coli was of the same batch that was used in the restaurant at the time of the outbreak. The patty had never been in either of the restaurants so it could not have been cross-contaminated in the restaurants, and this ruled out an infected food handler as the principal source. Furthermore, the contaminated patty was raw, indicating the cooking process had allowed the bacterium to survive and remain in the final product. The food production process was examined carefully and it was found that the grills in the implicated restaurants had not reached the specified temperatures during busy periods.
Following these two foodborne outbreaks, in November 1982 an outbreak of diarrhoea with haemorrhagic colitis affected thirty-one out of 353 residents of a home for the elderly in Ontario, Canada. E.coli O157 was isolated from eighteen individuals. Epidemiological investigations showed an association between the place of eating and illness, consistent with a contaminated food stored in warming ovens before being served to residents in their rooms and in a dining room somewhere away from the kitchen. Hamburgers had been served one to two days prior to the outbreak. An important aspect of this outbreak was the biphasic epidemic curve, a feature of secondary transmission, suggesting that O157 could be passed from person to person. Since then, person-to-person transmission, especially in nursing homes and between young children, has been an important feature of the epidemiology of the disease (Stewart et al.1983).
In 1982 when these outbreaks occurred it was not known how common a problem was posed by O157 and several research groups established population surveillance schemes aimed at establishing the extent of sporadic infection. The surveillance programmes soon established that sporadic cases of O157 occurred regularly, in addition to the occasional outbreaks, and that there was a wide geographical distribution in the USA, Canada and the United Kingdom. Surveillance also demonstrated that the range of clinical illnesses in those presenting with this infection was wider than the early outbreaks had suggested, and as well as haemorrhagic colitis, it included non-bloody diarrhoea, and in some cases a renal problem called haemolytic uraemic syndrome.
How VTEC causes illness in humans
Table 1.2 summarises the pathogenic mechanism of some common bacterial enteric pathogens.
To control VTEC O157, EHOs need an understanding of the ways in which it causes disease in humans. VTEC O157 possesses three potential virulence attributes: namely, ‘adherence’, ‘attachment-and-effacement’ and ‘production of vero cytotoxins’.
Adherence
Microbial adherence molecules (adhesins) allow some bacteria to adhere to the gut wall by attaching to receptors possessed by the cells lining the gastrointestinal tract. Attachment to the mucosal surface of the gut prevents the bacteria from being swept along by the natural peristaltic action and brings bacterial toxins into close contact with the eukaryotic cell surfaces.
VTEC O157 can adhere to the intestine of experimentally infected animals. Using animal and laboratory experiments on cell lines, some investigators have concluded that adherence is conferred by the 60MDa plasmid, possessed by all VTEC O157. Others have concluded that the adherence occurs via surface proteins (Dytoc et al. 1993; Karch et al. 1987; Levine 1987; Louie et al. 1993; Sherman et al. 1997; Tzipori et al. 1987; Wadolkowski et al. 1990).
Table 1.2 Pathogenic mechanisms of common bacterial enteric pathogens
Attachment-and-effacement
Attachment-and-effacement, though it has not been demonstrated in humans, has been described as a major morphological manifestation of VTEC O157 infection (Kelly et al. 1990). It has been described as an intimate bacterial attachment to the surface of enterocytes with the formation of a cup or pedestal from the cell surface, in which the bacterium sits. It has also been shown that non-O157 VTEC strains caused attaching-and-effacing lesions in experimentally infected rabbits.
Further evidence of the likelihood of attaching-and-effacing lesions in human E.coli O157 infection was provided by their similarity to lesions produced by EPEC. The attaching-and-effacing lesions associated with E.coli O157, and observed in animal experiments, were indistinguishable from the attaching-and-effacing lesions seen in humans and animals infected with EPEC strains (Moon et al. 1983; Tzipori et al. 1989).
VTEC strains cured of their vero cytotoxin associated bacteriophage and hence unable to produce VT have caused diarrhoea in monkeys (Tzipori et al. 1989). Also, some E.coli O157 isolated from humans with diarrhoea have been found not to produce VT. The diarrhoea was believed to be caused by the attaching-and-effacing mechanism.
Recent evidence has indicated that VTEC can invade certain human epithelial cell lines (T24 bladder and HCT-8 ileocecal) and that the invasion potential is chromosomally encoded (Oelschlaeger et al. 1994).
Toxin-production
VTEC O157 produces vero cytotoxin, so-called after the first demonstration of their toxicity on vero cells (African green monkey kidney cells). The VT produced by VTEC is indistinguishable from that produced by Shigella dysenteriae.
Low-level VT production has also been observed in non-pathogenic E.coli strains (K12) and other bacteria. An outbreak of severe gastroenteritis, HUS and TTP has been attributed to a vero cytotoxin producing strain of Citrobacter freundii.
It is now recognised that human isolates of VTEC O157 can, in fact, produce either or both of two vero cytotoxins which are termed VT1 and VT2.
VT1 is neutralised by antiserum against purified Shiga toxin produced by Shigella dysenteriae type 1. VT2 is not neutralised by the above. VT1 and VT2 are encoded by separate, identifiable bacteriophages. Variant forms of VT2, commonly referred to as VTv, have also been reported, which are not ‘phage-encoded.
The toxins consist of an A (active) and multiple copies of a B (binding) subunits. The B subunit must bind to a receptor for the toxin to exert its pathogenic effect. The receptor for most VTs is a glycolipid globotriaosyl ceramide (Gb3) present on the surface of susceptible cells. The A subunit then enters the cell and inhibits protein synthesis. It is currently thought that VTs kill the epithelial cells lining the colon which leads to fluid secretion into the gut and hence to diarrhoea. Furthermore, damage of the blood vessels of the colon gives the blood seen in the faeces. The Gb3 receptor for VT is present in human renal tissue and the putative target of VT, during the development of HUS, is believed to be the renal glomerular microvascular endothelial cells. The damage caused to the renal glomerular endothelium is likely to affect haemostasis, leading to occlusion of the glomerular microvasculature by platelets and fibrin.
Various laboratory animal models have been extensively used to demonstrate the toxicity of purified vero cytotoxin on the intestine, kidneys and central nervous system. There is further evidence that VT plays a role in the pathogenesis of VTEC O157 disease. Free VT has been identified in the faeces of patients with VTEC O157 infection. Antibodies to VT have also been demonstrated in infected individuals. Furthermore, many different VTEC strains are isolated from patients with HUS indicating that the common pathogenic mechanism is production of VT.
Animal models have indicated that, where VTEC O157 infection involves a strain that produces VT2, the likelihood of HUS developing is greater although evidence as to the reasons for this are conflicting and beyond the scope of this book. Nevertheless, human studies have also shown that individuals who develop HUS are infected with a strain which produces VT2. To summarise, VTEC O157 causes illness in humans by initially adhering to the lining of the colon and then forming an attaching-andeffacing lesion. The organism produces one or both of two vero cytotoxins. The resulting damage to the epithelial cells causes secretion of fluid into the lumen of the gut and an initially watery diarrhoea. Further damage to small blood vessels causes blood to be seen in the stool. In some individuals the VT becomes bloodborne and affects capillaries in the kidneys causing kidney failure. VT2 is more important in the development of HUS than VT1.
Incubation period
The incubation period for VTEC O157 cannot be directly ascertained from volunteer studies. It can, however, be estimated from outbreaks where a point source of infection, and hence an exact time of exposure, can be identified.
The usual incubation period is...
Table of contents
- Cover page
- Other books in clay’s library of health and the environment:
- Title page
- Copyright page
- Clay’s library of health and the environment
- Acknowledgements
- Abbreviations
- Chapter 1: Overview
- Chapter 2: How is VTEC diagnosed?
- Chapter 3: How common is VTEC infection?
- Chapter 4: How does VTEC spread to humans?: Evidence from sporadic cases
- Chapter 5: How does VTEC spread to humans?: Evidence from outbreaks
- Chapter 6: Animal and environmental reservoirs of VTEC
- Chapter 7: Control of VTEC O157
- Glossary
- Useful contact telephone numbers, addresses and websites
- Bibliography
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access E.coli by Stephen Palmer,Sharon Parry in PDF and/or ePUB format. We have over 1.5 million books available in our catalogue for you to explore.