Decision-making pervades all aspects of midwifery practice across the world. Midwifery is informed by a number of decision-making theories, but it is sometimes difficult to marry these theories with practice.
This book provides a comprehensive exploration of decision-making for midwives irrespective of where in the world they practice or in which model of care. The first part critically reviews decision-making theories, including the Enhancing Decision-making Assessment in Midwifery (EDAM) tool, and their relevance to midwifery. It explores the links between midwifery governance, including professional regulation and the law, risk and safety and decision-making as well as how critical thinking and reflection are essential elements of decision-making. It then goes on to present a number of diverse case studies, demonstrating how they interrelate to and impact upon optimal midwifery decision-making. Each chapter presents examples that show how the theory translates into practice and includes activities to reinforce learning points.
Bringing together a diverse range of contributors, this volume will be essential reading for midwifery students, practising midwives and midwifery academics.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Part I Influencing factors underpinning midwives’ decision-making
1 Midwifery and decision-making theories
Elaine Jefford
Chapter overview
The focus of this chapter will be on the following decision-making theories/models and frameworks/tools: medical clinical reasoning, a non-midwifery specific shared decision-making model (USA and UK), a midwifery-specific decision-making model (UK), decision-making tool (Australia and UK), decision-making flowchart (Ireland) and Page’s (UK) five steps of evidence-based midwifery. These will be critically appraised for their ability to provide a teachable framework for midwifery clinical reasoning that is consistent with the philosophy of midwifery and their utility to midwifery practice.
Introduction
The International Confederation of Midwives (ICM) represent approximately 500,000 midwives across 113 countries via its 132 midwives associations. The ICM mandates the required level of education, professional responsibilities and clinical skills a midwife is to demonstrate, irrespective of geographical location or model of care. The ICM’s explicit aim is to promote and safeguard the safety of women and babies, thus holding midwives to account for their clinical reasoning, decisions, resultant actions and any related outcomes (International Confederation of Midwives, 2017, 2018). This accountability has been accepted and incorporated in many countries’ regulatory documents, such as Australia (Nursing and Midwifery Board of Australia, 2018b), the UK (Nursing and Midwifery Council, 2014), New Zealand (Midwifery Council New Zealand, 2007, 2010), Iceland (Ministry of Welfare, 2012), and the Netherlands (Gezondheidszorg, 1993; Verloskundige, 2008), but yet not in others, for example Mexico, Bangladesh and India. Although outside the scope of this chapter, it is worth acknowledging midwifery decision-making accountability has not transferred into practice within some countries, such as in Central and Eastern Europe (Mivsek et al., 2016).
There are numerous decision-making theories, models, frameworks, tools and aids within the disciplines of medicine and nursing. In the past, midwifery has drawn upon these as well as from other disciplines. Yet how well suited they are to midwifery is debatable. In 2011, Jefford, Fahy and Sundin explored the strengths and limitations of several decision-making theories/framework and their usefulness to midwifery (Jefford et al., 2011). This paper drew on Jefford’s (2012) PhD thesis. The authors of the paper and Jefford concluded no decision-making theories embraced the midwifery philosophy so could not meet the needs of midwifery (Jefford et al., 2011; Jefford, 2012). The information presented in those publications remains relevant to midwifery today, despite the passage of time.
As new context-specific knowledge has emerged and the landscape of contemporary midwifery has changed, it is timely to explore more recent decision-making theories/models and frameworks as well as to revisit two older ones. The first part of this chapter will briefly refer to medical clinical reasoning and present a synopsis of a non-midwifery-specific shared decision-making model (USA and UK). This will be followed by a midwifery-specific decision-making model (UK), a decision-making tool (Australia and UK), a decision-making flowchart (Ireland) and Page’s (2000, 2006) five steps of evidence-based midwifery (UK). The second part of the chapter will be a critical appraisal of these for their ability to provide a teachable framework for midwifery clinical reasoning that is consistent with the philosophy of midwifery and their utility to midwifery practice. The final part of the chapter will offer the reader an opportunity to engage in a clinical reasoning learning activity.
Medical clinical reasoning
Medical clinical reasoning derives from the analytical or rational approach to decision-making – hypothetico-deductive theory. As such, this theory and medical clinical reasoning favours the technical rational approach, relying on empirical data such as randomised controlled research and quantifiable clinical data obtained from the five senses. Over time it’s clearly defined steps, albeit with slight variations, have been well documented (Elstein et al., 1978; Elstein and Schwartz, 2000; Elstein et al., 1978; Jefford et al., 2011, 2016; Chodzaza et al., 2018). The clinical reasoning steps are documented in a linear way and consist of:
Cue acquisition
Cue clustering
Cue interpretation or hypothesis generation
Focused cue acquisition
Diagnosis
Evaluate treatment options
Implement or prescribe treatment
Evaluate treatment outcomes.
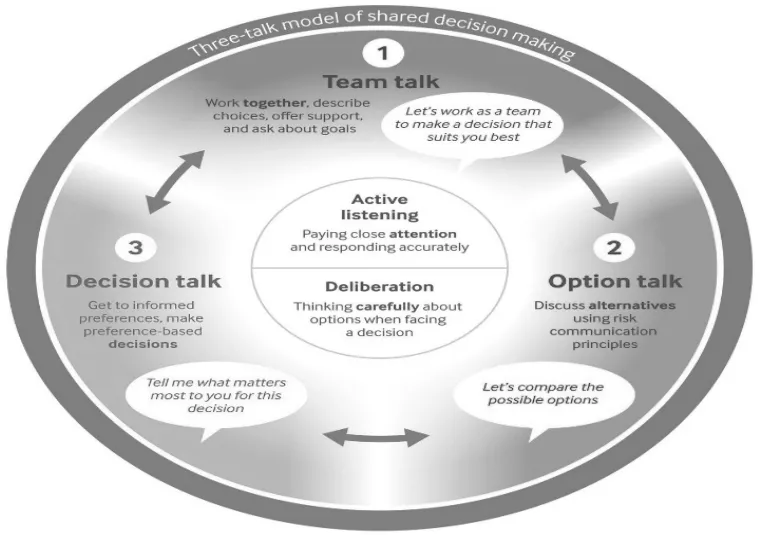
Three-talk model for shared decision-making
This model was first published in 2012 (Elwyn et al., 2012) and revised in 2017 following feedback. The original model was linear and lacked elements around risk, patient preferences and the relational psychosocial dimensions of care (Elwyn et al., 2017). Medical practitioners are the intended audience of this model. Yet as you will see as you read different chapters within this book, midwives are using it.
The three-talk model for shared decision-making has three key steps embedded within an active listening and deliberation ethos: Team Talk, Option Talk and Decision Talk. The aim of the Team Talk step is to establish what outcomes the patient wants around their health. The medical practitioner then offers ‘reasonable options’ of care provision using a variety of media such as email. Discussion led through risk communication principles guide the next step: Option Talk, which is a collaborative, reciprocal, face-to-face meeting between the medical practitioner and the patient. Care options are reviewed, patient understanding is clarified and a patient decision support tool is utilised. The final step in this shared decision-making model is Decision Talk. Medical practitioners elicit what matters and what is valued by the patient and how this fits within the decided upon care provision option.
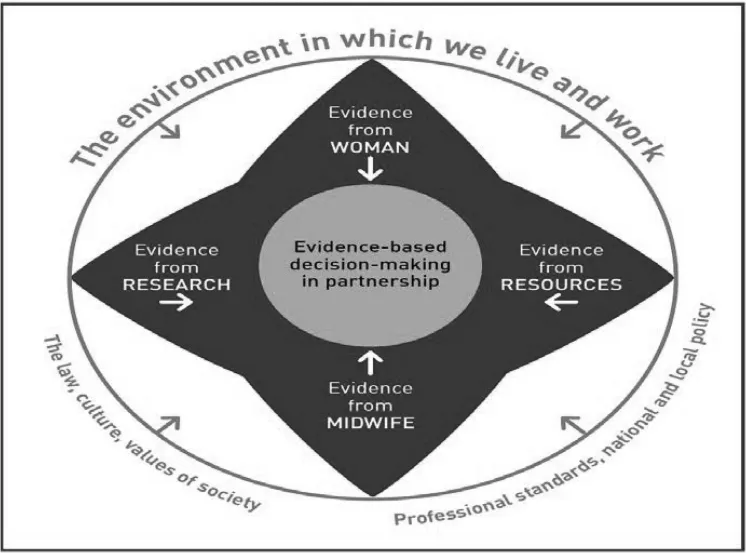
This midwifery-specific decision-making model sits within the physical, legal, political, cultural and societal environmental boundaries within which women and midwives live and work. This includes midwifery professional standards and national and local policies. These elements influence the four areas of evidence: from the woman, from resources, from the midwife and from research, which in turn impact upon the partnership evidence-informed decision-making at the centre of the model (Menage, 2016a, 2016b).
Evidence from the woman has three components: (1) a midwife employing a technical rational approach gathering quantifiable clinical data using her/his five senses; (2) a midwife exploring and understanding what the woman’s psychological and social health is and her needs; (3) establishing a reciprocal woman/midwife partnership based on equality. Evidence from resources focuses on the midwife’s knowledge about the boundaries or scope of practice each member of a multidisciplinary team has and the ability to access such professionals. It also requires the midwife to have the capability and capacity to draw on her knowledge in order to offer the woman a multidisciplinary care approach as and when necessary. Encapsulated within the evidence from midwife area is time to enable a dialogue so informed decisions can be made. A midwife’s need to reflect on her/himself as a professional and person, including any limitations and how these impact upon her/his role within the woman/midwife partnership, is also noted to be an important part of this area of evidence. Evidence from research relies on qualitative and quantitative research as well as evidence from the other three areas of this model.
Figure 1.1 Three-talk model for shared decision-making
Enhancing Decision-making and Assessment in Midwifery (EDAM)
This midwifery specific decision-making tool arose from etic and emic data. Midwives from all states and territories in Australia representing all models of maternity care provision were part of an original decision-making framework (Jefford, 2012). Etic data was drawn from theoretical literature around decision-making, for example Hamm (1988a, 1988b) and Hammond (1980) and specifically medical clinical reasoning (Elstein et al., 1978; Elstein and Schwartz, 2000; Elstein et al., 1978, Jefford et al., 2011, 2016; Chodzaza et al., 2018), birth territory theory (Fahy et al., 2008) and midwifery professional, regulatory and legal documents (International Confederation of Midwives, 2011, 2017, 2018; Nursing and Midwifery Board of Australia, 2018a, 2018b).
In 2016, following international testing, the original Jefford (2012) decision-making framework was changed and EDAM (Jefford et al., 2016) was born. EDAM (Jefford et al., 2016) has been verified as a robust, valid and reliable psychometric instrument for measuring midwifery decision-making.
Figure 1.2 A model for evidence-based decision-making in midwifery
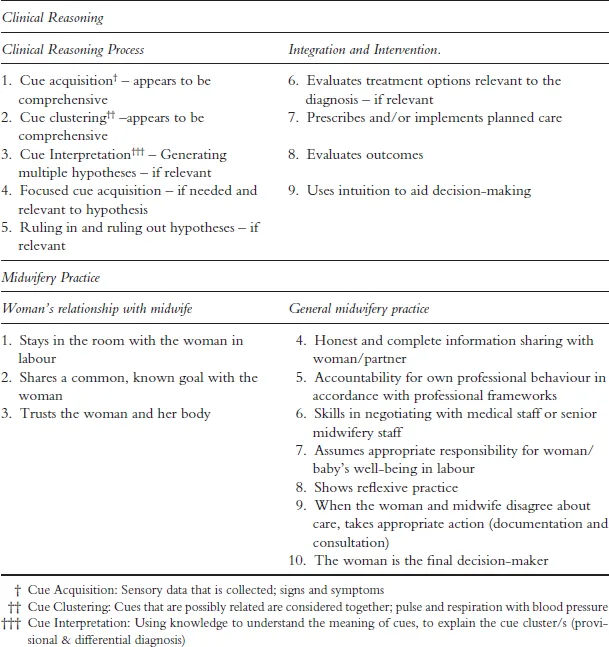
EDAM has two domains: Clinical Reasoning and Midwifery Practice. The Clinical Reasoning domain reflects the steps of medical clinical reasoning as noted earlier. Yet unlike medical clinical reasoning it has two distinct subscales: the clinical reasoning process emphasises the theoretical aspect of hypothetico-deductive theory and arriving at a hypothesis, whilst the integration and intervention subscale focuses more on nursing models of clinical reasoning and the inclusion of intuition and reflection.
The Midwifery Practice domain embraces the midwifery philosophy within the boundaries of midwifery professional frameworks (International Confederation of Midwives, 2011, 2017, 2018). The subscale women’s relationship with the midwife centres on knowing what matters and what is important to the woman, trusting the physiological process of birth and being present with the woman – in other words, the philosophy of midwifery (International Confederation of Midwives, 2014a). General midwifery practice links with how the midwife enacts the professional frameworks to support decision-making.
Table 1.1 Clinical reasoning
Scope of practice decision-making flowchart
This type of flowchart is not unique to Ireland, with countries such as Australia (Nursing and Midwifery Board of Australia, 2010) and the Netherlands (Expertgroep Zorgstandaard Integrale Geboortezorg Expertteam Care standard Integral Maternity Care, 2016) offering versions which focus on decision points. For this section, however, the Nursing and Midwifery Board of Ireland has a decision-making flowchart within their Scope of Nursing and Midwifery Practice Framework (Nursing and Midwifery Board of Ireland, 2015), which was why it was chosen by the author. This framework is encased within midwifery professional documents such as the Code of Professional Conduct and Ethics for Registered Nurses and Registered Midwives and the Scope of Practice framework (Nursing and Midwifery Board of Ireland, 2014, 2015). The flowchart aims to ensure patient safety by posing key questions which ask nurses and midwives to accept responsibility and accountability for their role and/or activity including collaboration or referral to other healthcare providers. It does this through four key questions:
1 Does the role/activity sit within the values and definitions of the (above) professional documents?
2 Are you competent to perform the role/activity?
3 Is this role/activity support by the clinical environment (legislation, policy, evidence)?
4 Are you willing to accept responsibility and accountability for your role and/or activity?
The nurse/midwife may proceed if these questions are answered positively. If the answer is negative at any step, then collaboration or referral to other healthcare providers is required.
Five steps of evidence-based midwifery
In 2000, Page (2000) put forward these five steps with the aim of interlinking the sensitivity (art) and scientific evidence (science) within midwifery. In 2006, Page (2006) again published her five steps using a scenario to illustrate how to apply it (pp. 360–371). Although Page (2000, 2006) does not explicitly refer to the five steps of evidence-based midwifery as a decision aid, it is considered as one by many midwives. The rationale is that in order to provide evidence-informed care, a midwife must enter into a relationship whereby a sharing of information occurs, thus enabling the woman to be the decision-maker about her care. During such sharing, the midwife must engage in these five steps:
1 Finding out what is important to the woman and her family
2 Using information from the clinical examination
3 Seeking and assessing evidence to inform decisions
4 Talking it through
5 Reflecting on the outcomes, feeling and consequences (Page, 2006, p. 360).
Having read the brief synopsis of the other theories/models and frameworks descriptions, it becomes evident that they and the five steps offered by Page (2000, 2006) are intrinsically linked.
Strengths and limitations of the presented decision-making theories/models and frameworks
Decision-making is complex, multi-dimensional and influenced by multiple factors. Within midwifery, unlike other professions, an added complexity is the mother-baby dyad. Any decision made ultimately has the potential to impact upon not only the childbearing women (hereinafter referred to as the woman), but also her (unborn) baby. Midwifery acknowledges and embraces a woman’s autonomy and the need for her to be central in all decision-making (International Confederation of Midwives, 2014a; Department of Health, Public Health England, 2014).
Global healthcare reforms focus on a people-centred healthcare approach (World Health Organization, 2007). This has led to changing societal expectations of ...
Table of contents
Cover
Half Title
Title
Copyright
Dedication
Contents
List of illustrations
List of contributors
Foreword
Introduction
Part I Influencing factors underpinning midwives’ decision-making
Part II Translating theory into practice
Part III Decision-making within the context of the socially and culturally constructed maternity care environment
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Empowering Decision-Making in Midwifery by Elaine Jefford, Julie Jomeen, Elaine Jefford,Julie Jomeen in PDF and/or ePUB format, as well as other popular books in Medicine & Ethics in Medicine. We have over 1.5 million books available in our catalogue for you to explore.