eBook - ePub
Diagnosis of Non-accidental Injury
Illustrated Clinical Cases
- 337 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Diagnosis of Non-accidental Injury
Illustrated Clinical Cases
About this book
Recognition and diagnosis of child abuse and neglect creates an important foundation for the protection of children. Physicians and other healthcare providers have a fundamental role in this process, and need to be confident that they can identify correctly the signs and symptoms that provide clues to non-accidental injuries resulting from child ma
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicinaCASE 1
This Asian 6-year-old boy was removed from his mother’s care when police were called to his house by the neighbours. They reported hearing him screaming and saw his mother running after him with ‘a stick’. He was brought to the emergency room where lesions were found on his body (Image 1a). There was no medical history available from the child or protective services worker. He refused to disclose what happened. His mother was taken into police custody, where she said that she was punishing him for poor marks on his first-grade report card. She reported that she and her child recently emigrated from China and she believed in physical discipline, having used this several times before to modify his bad behaviour. She reported that he has no chronic diseases, did not bleed easily and did not take any medication. She also denied using any home remedies or other alternative treatments at home.
i. |
What does the image show?
|
ii. |
Does the reported physical discipline explain the lesions?
|
iii. |
Are there cultural factors present that would modify your assessment about whether this child was abused?
|


i. |
There are multiple marks of varying colour depicted over his back. Most are irregularly shaped bruises with red and yellow colour and some have thin eschar suggesting healing abrasion or laceration. While the image is limited, it does not appear that the child is malnourished or has other chronic skin conditions or scars. The remainder of the examination is normal.
|
ii. |
The marks as initially depicted are difficult to characterize as to cause. An object such as a stick is possible. Further information is obtained from closer inspection of one of the lesions (Image 1b). This shows two lines evenly spaced with some erythema. The police also bring you the ‘stick’ which was being used which appears to be a stalk of bamboo with similar diameter. This led you to conclude that the reported discipline was consistent with the lesions.
|
iii. |
Different laws and regulations in different jurisdictions govern the legal interpretation of responsibility when injuries arise from physical discipline, also called corporal punishment. As guidance for the medical assessment, the American Academy of Pediatrics (AAP) has noted that corporal punishment is of limited effectiveness and has potentially deleterious side effects.1 The AAP recommends that parents be encouraged and assisted in the development of methods other than spanking for managing undesired behaviour in children. Using time-out, removal of privileges and punishment are common discipline approaches that have been associated with reducing undesired behaviour. These different strategies, sometimes confusingly called ‘punishment’, are effective if applied appropriately to specific behaviours. In this case, the mother reported that bamboo is often used for this purpose among people from her culture and that she had not learned about other techniques. To the extent that these lesions were inflicted upon the child, they constitute physical abuse. However, any treatment or remediation plan should take these cultural influences into account.
|
1. American Academy of Pediatrics Committee on Psychosocial Aspects of Child and Family Health. Guidance for effective discipline. Pediatrics. 1998;101(4 Pt 1):723–728.
CASE 2
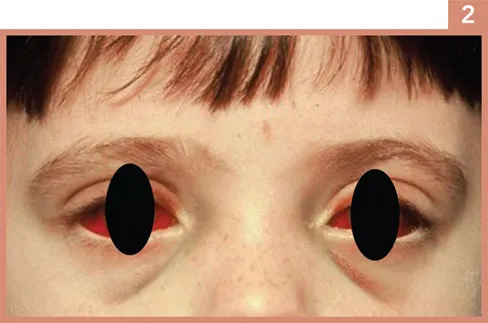
This 3-year-old child was brought to the emergency department in the middle of the night by her grandmother. She said the girl was fine when she went to bed. She heard the child coughing in the night and when she checked her, the girl looked like this (Image 2).
i. |
What signs do you notice?
|
ii. |
What history would you take?
|
iii. |
What is the differential diagnosis?
|
i. |
The girl has bilateral subconjunctival haemorrhages with ecchymoses of the upper and lower eyelids and a slight degree of congestion and oedema of the orbit. She also has fine petechiae of the face.
|
ii. |
The doctor needs to take a full medical history, in particular asking details of the nature of the cough. A social history should also be taken and health and social care records checked for previous safeguarding concerns.
|
iii. |
Child abuse has been recognized as a cause of subconjunctival haemorrhage. Cases with non-accidental intracranial injury and fractures have presented with a single small unilateral haemorrhage when further investigations such as brain imaging and skeletal survey are done. Other causes of subconjunctival haemorrhage include blood dyscrasias and coagulopathies, malignancies such as metastatic neuroblastoma or rhabdomyosarcoma and leukaemia, conjunctivitis and traumatic asphyxia from severe chest compression. Bouts of violent coughing in pertussis, as in this case, were well recognized as a cause of severe subconjunctival haemorrhages when the infection was more common. However, the presence of pertussis does not rule out non-accidental injury, so appropriate assessments should still be undertaken in suspicious cases.1–3
|
1. Lowe L, Rapini RP, Johnson TM. Traumatic asphyxia. J Am Acad Dermatol. 1990;23(5 Pt 2):972–974.
2. Paysse EA, Coats DK. Bilateral eyelid ecchymosis and subconjunctival hemorrhage associated with coughing paroxysms in pertussis infection. J Aapos. 1998;2(2):116–119.
3. Spitzer SG, Luorno J, Noel LP. Isolated subconjunctival hemorrhages in nonaccidental trauma. J Aapos. 2005;9(1):53–56.
CASE 3
Child Protective Services referred this 9-month-old baby girl to the emergency department. She started at a new daycare that morning, and they were concerned about multiple bruises on her back. She has been previously healthy and is asymptomatic. Image 3 shows her back and buttocks. The remainder of her examination was normal.

i. | What is your diagnosis? |
This child has dermal melanosis (commonly called Mongolian spots) on her back and buttocks. They were thought to be bruises inflicted by her daycare provider. Dermal melanosis refers to congenital hyperpigmented lesions more commonly seen in black, Asian, Latino and Native American infants but can occur in any infant. In most cases, lesions are located on the buttocks, lumbosacral region, back and shoulders as in this infant.1 The spots have variable sizes, shapes and colour but are typically blue-grey or blue-green patches with irregular borders and, thus may be confused with bruises.1 In this infant, they were documented at birth on her delivery records and her mother stated she ha...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Preface
- Broad Classification of Cases
- Contributors
- Image Contributors
- Case 1
- Case 2
- Case 3
- Case 4
- Case 5
- Case 6
- Case 7
- Case 8
- Case 9
- Case 10
- Case 11
- Case 12
- Case 13
- Case 14
- Case 15
- Case 16
- Case 17
- Case 18
- Case 19
- Case 20
- Case 21
- Case 22
- Case 23
- Case 24
- Case 25
- Case 26
- Case 27
- Case 28
- Case 29
- Case 30
- Case 31
- Case 32
- Case 33
- Case 34
- Case 35
- Case 36
- Case 37
- Case 38
- Case 39
- Case 40
- Case 41
- Case 42
- Case 43
- Case 44
- Case 45
- Case 46
- Case 47
- Case 48
- Case 49
- Case 50
- Case 51
- Case 52
- Case 53
- Case 54
- Case 55
- Case 56
- Case 57
- Case 58
- Case 59
- Case 60
- Case 61
- Case 62
- Case 63
- Case 64
- Case 65
- Case 66
- Case 67
- Case 68
- Case 69
- Case 70
- Case 71
- Case 72
- Case 73
- Case 74
- Case 75
- Case 76
- Case 77
- Case 78
- Case 79
- Case 80
- Case 81
- Case 82
- Case 83
- Case 84
- Case 85
- Case 86
- Case 87
- Case 88
- Case 89
- Case 90
- Case 91
- Case 92
- Case 93
- Case 94
- Case 95
- Case 96
- Case 97
- Case 98
- Case 99
- Case 100
- Case 101
- Case 102
- Case 103
- Case 104
- Case 105
- Case 106
- Case 107
- Case 108
- Case 109
- Case 110
- Case 111
- Case 112
- Case 113
- Case 114
- Case 115
- Case 116
- Case 117
- Case 118
- Case 119
- Case 120
- Case 121
- Case 122
- Case 123
- Case 124
- Case 125
- Case 126
- Case 127
- Case 128
- Case 129
- Case 130
- Case 131
- Case 132
- Case 133
- Case 134
- Case 135
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Diagnosis of Non-accidental Injury by Vincent J. Palusci, Dena Nazer, Patricia Brennan, Vincent J. Palusci,Dena Nazer,Patricia Brennan in PDF and/or ePUB format, as well as other popular books in Medicina & Medicina d'urgenza e terapia intensiva. We have over 1.5 million books available in our catalogue for you to explore.