eBook - ePub
Information and Communication Technologies in Healthcare
- 264 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Information and Communication Technologies in Healthcare
About this book
As the population ages and healthcare costs continue to soar, the focus of the nation and the healthcare industry turns to reducing costs and making the delivery process more efficient. Demonstrating how improvements in information systems can lead to improved patient care, Information and Communication Technologies in Healthcare explains how to cr
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Subtopic
ManagementIndex
Computer Science1
HEALTHCARE SYSTEMS
Introduction
FRANK M. GROOM, PH.D.
Contents
Central Data Repositories
Data Information Entry, Verification, and Correction
Regional Sharing of Information
Data Privacy and Protection
Open Systems
Compliance
Conclusion
Areas Covered by This Book
References
As the population ages, the economy struggles, and healthcare costs soar, the focus of the nation and the Healthcare Industry is on determining the means to reduce costs and make the delivery process more effective. Systems experts are like carpenters in their view of these problems. To a carpenter, every information problem appears solvable with nails and a hammer (or screws and screwdriver, or at least a little carpenter’s hide or wood glue). To information technology people, solutions frequently involve collecting data into a repository and then making it searchable, understandable, and relatable.
In this book, we approach the healthcare industry and its problems from an Information Systems prospective and attempt to determine how to create a helpful and holistic Medical Records System as a core component to be employed in addressing a wide range of healthcare issues. A basic principle we flow is that data should be captured only once, stored in a repository, and then made available throughout the medical system for all medical purposes.
Such a Medical Records System Data Repository starts with a record created by a patient’s physician. Furthermore, additional records of request are sent by the patient’s physician for any tests and procedures that the physician determines must be undertaken and any specialists to whom the patient is referred. For an efficient systems process, a patient’s information file from that physician’s office should initially be forwarded into a common record-keeping system. All further information from other healthcare providers can subsequently be entered into a common file and updated with hospital, specialist, and further diagnostic and performed procedures. Any additional patient, symptom, and planned procedures can be inserted in an existing medical record that has previously been standardized, edited, and vetted for completeness by an initial medical provider and need not be re-entered at each subsequent registration time.
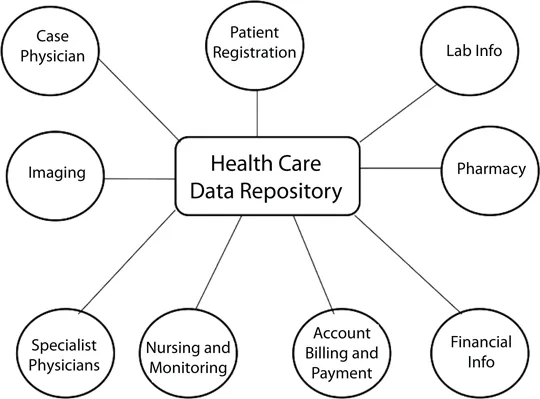
For each patient, from the time of physician prescribing a medication or ordering a set of tests, specialist evaluations, or full hospitalization, an Electronic Case Report (ECR) should be prepared and stored in a common repository. This ECR should then follow the patient throughout the healthcare process, office to office, doctor to doctor, with information accumulating as the process proceeds. The updated ECR should be stored in the central Health Care Data Repository (HCDR) (Figure 1.1) as the patient proceeds through each step of the medical process. Providers access a common patient ECR record, and subsequently update it with the additional information gathered from that stage’s processes. The accumulated set of patient information always remains in the central (HCDR) storage.
Central Data Repositories
Initial versions of such a central repository are currently deployed in a number of specialized centers. As an example of such a repository, the Clinical Data Repository/Health Data Repository (CHDR)2 is a joint initiative between the Department of Veterans Affairs (VA) and the Department of Defense (DoD). Another example is AHLTA (Armed Forces Health Longitudinal Technology Application), an enterprisewide medical and dental information management system that provides secure online access to Military Health System (MHS) beneficiary records. To achieve computable interoperability, both agencies standardize their data for each given clinical domain (pharmacy, allergy, etc.) and exchange the standardized data through a common interface.
Thus, the CHDR repository consists of an interface between the DoD’s Clinical Data Repository (CHDR), the AHLTA repository, the DoD’s electronic health record, and the VA’s Health Data Repository (HDR). The CHDR is thus a Cross-Government Department Data Repository that enables the bi-directional exchange of patient, pharmacy and medication, and allergy data. Furthermore, common usage of the CHDR enhances decision support by permitting data from VA and DoD repositories to be cross-referenced for drug-to-drug interactions and drug-allergy effects.
The CHDR is an important step forward toward system and provider interoperability and represents a departure from a “viewable” data approach. Instead of healthcare providers merely being empowered to a have a common view of the patient data, the data is only entered and stored once and does not merely appear the same to all providers but is in fact only a single common record in a common file. By employing an agreed-upon “vocabulary” for their data and thus a common procedure naming convention, the VA and the DoD have standardized their data so that they can to use each other’s data in decision support applications and in making medical decisions and reaching common medical conclusions.
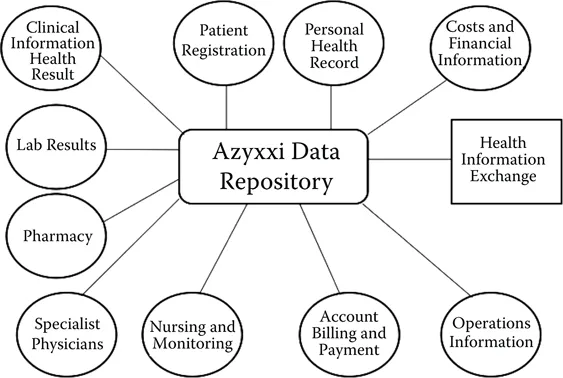
Another Data Repository System, Microsoft’s Azyxxi Data Repository, was developed by a group of doctors and initially used in Washington Hospital Center’s emergency department beginning in 1996. Microsoft subsequently purchased the system from these doctors. The University of Washington currently employs the system, now called the Azyxxi Data Repository system, to centralize all information associated with their Pain Control Clinic. The Azyxxi Data Repository system has since been deployed at six other hospitals, among which are Georgetown University Hospital and the MedStar Health group, a nonprofit network in the Baltimore-Washington region.
In addition to storing basic patient information, the Azyxxi software and associate Data Repository system is designed to retrieve and quickly display information from many sources, including scanned documents, EKGs, x-rays, MRI scans, angiograms, and ultrasound images (Figure 1.2). Essentially, the Azyxxi Data Repository is an advanced multimedia, object-oriented database system with user-oriented interfaces, displays, and search engines.
There are several more established suppliers of clinical information technology systems, including Cerner, Epic, G.E., Eclypsis, and others. A current list of software vendors providing healthcare data repository software systems is available by means of Google search or Wikipedia.
Data Information Entry, Verification, and Correction
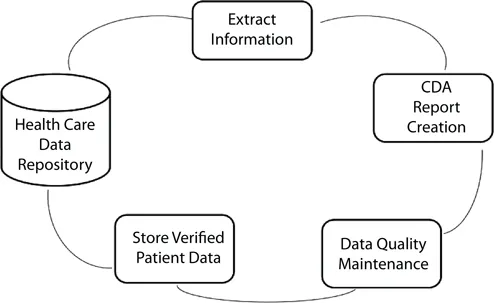
Although a common, central repository is critical, additional subsystems are required for each of the groups and organizations that will use data in the repository. A standardized report system should be created with a format and vocabulary that is understood by all information users. Furthermore, a patient data verification process should be conducted whenever a patient has any medical procedure performed. Additionally, an overall information quality assurance procedure should be performed against the stored data on a regular basis (Figure 1.3).
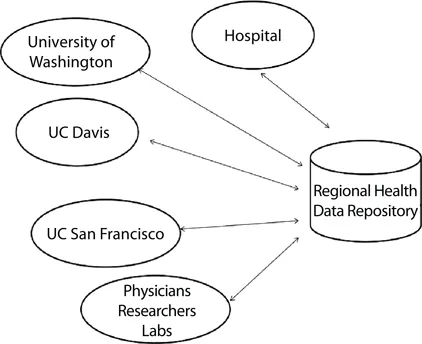
Regional Sharing of Information
It is important that all medical facilities in a region have access to a commonly stored and shared information set. This commonality ensures that a least cost data acquisition, verification, and storage processes are employed for all users in a given area without duplication, variation, or proprietary restrictions. Such an example is contained in Figure 1.4 from the West Coast.
Data Privacy and Protection
When multiple people within a physician’s office, hospital, support facility, and imaging and laboratory sites have access to a common shared Health Care Record System, many opportunities exist for misuse of the data by people with malicious or inappropriate intent. Federal and state laws have been enacted to enforce the privacy of such records. The operators of a common Health Care Records System must carefully follow such regulations. These measures include restriction as to access, both at the device and at the system level. These may include encrypting the data, employing and frequently changing passwords, requiring the use of authentication and certification systems, employing tracking systems, and the maintenance of a support team that is trained and experienced with the system and the deployed technologies.
Open Systems
Medical Information Systems have been plagued by a number of issues. They have frequently been built by small companies with limited financial stability. They tend to be designed for a specific specialized need and limited user group. They frequently have been developed with a proprietary programming system, deployed to operate on proprietary hardware and software, and based upon a limited data management and storage system.
This proprietary situation may be difficult to address. For example, the various scanning and imaging devices that exist may produce records of results that are in a proprietary format associated with the hardware deployed. That imaging information could possibly limit the ability to directly enter the resulting data into a central repository system written with standard C, C++, COBOL, or other commonly used software, or with an operating system of Unix, Linux, Windows®, MVS (IBM’s Multiple Virtual Storage now called Z/OS), VM (IBM’s Virtual Machine now called Z/VM), or other generally deployed operating systems. As a result, an organization that employs such systems frequen...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- CONTRIBUTORS
- CHAPTER 1 HEALTHCARE SYSTEMS: INTRODUCTION
- CHAPTER 2 TECHNOLOGY AS A CATALYST FOR HEALTH ENHANCEMENT
- CHAPTER 3 HEALTH INFORMATION EXCHANGE
- CHAPTER 4 UNIVERSAL DATA STANDARDS
- CHAPTER 5 HEALTHCARE INFORMATION EXCHANGE
- CHAPTER 6 HEALTH INFORMATION TECHNOLOGY IN THE UNITED STATES: ACHIEVING LEGAL AND REGULATORY RESULTS THAT ENHANCE INNOVATION AND ADOPTION
- CHAPTER 7 HEALTHCARE REGULATIONS, PRIVACY, SECURITY, AND INFORMATION AGE CONSIDERATIONS
- CHAPTER 8 USABILITY: PATIENT–PHYSICIAN INTERACTIONS AND THE ELECTRONIC MEDICAL RECORD
- CHAPTER 9 REMEMBERING HUMAN FACTORS WHEN IMPLEMENTING TECHNOLOGY USE: A CASE STUDY IN HOME HEALTHCARE USABILITY
- CHAPTER 10 SECURITY AND PRIVACY: IMPACTS OF EVOLVING TECHNOLOGIES AND LEGISLATION
- CHAPTER 11 NEW FACILITY PLANNING: A HEALTHCARE FOCUS
- CHAPTER 12 DEVELOPING INNOVATIVE HEALTH INFORMATION FOR YOUTH: COMMUNICATION THEORY FOR PRACTICAL EMERGING MEDIA APPLICATIONS
- CHAPTER 13 RE-ENVISIONING THE INDIANAMEDICAID.COM WEBSITE AS A MEMBER-FOCUSED PORTAL: A CASE STUDY ON USABILITY AND TECHNOLOGY FOR TRANSFORMING HEALTHCARE COMMUNICATION
- APPENDIX: GLOSSARY OF HEALTH CARE TERMS FROM IBM
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Information and Communication Technologies in Healthcare by Stephan Jones, Frank M. Groom, Stephan Jones,Frank M. Groom in PDF and/or ePUB format, as well as other popular books in Computer Science & Management. We have over 1.5 million books available in our catalogue for you to explore.