Anorexia and bulimia nervosa: The terms
This chapter offers a comprehensive and accessible account of eating disorders. The term ‘eating disorders’ refers to a broad group of disorders, which includes anorexia nervosa, bulimia nervosa, obesity, binge eating, extreme dieting, fasting–bingeing cycles and other forms of subclinical anorexia and bulimia nervosa. By ‘eating disorders’ I will, however, mainly intend anorexia nervosa and bulimia nervosa (I will often use ‘anorexia’ and ‘bulimia’ to refer to ‘anorexia nervosa’ and ‘bulimia nervosa’), which are those eating orders mainly considered in the clinical literature.1 I shall, however, also discuss briefly what these other eating disorders, such as binge eating, are. The points raised on anorexia and bulimia nervosa can help with a more general understanding of other (sometimes less extreme) forms of disordered eating.
Anorexia nervosa
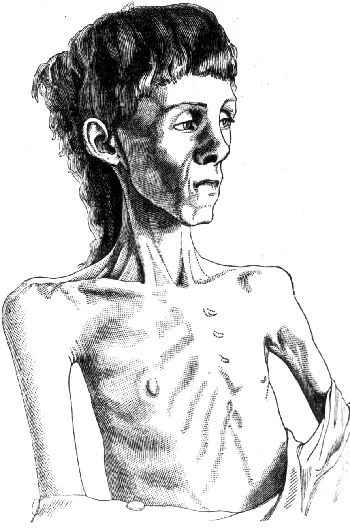
The term ‘anorexia nervosa’ was coined by William Gull in 1873. In 1888 this illustration appeared in his article ‘Anorexia Nervosa’, published in the Lancet.2 However, this phenomenon was noticed much earlier by Richard Morton, in London. In the Treatise of Consumptions (1694), he talked of:
Anorexia is a word of Greek origins, and literally means lack of appetite. Contrary to what the name originally denoted, anorexia nervosa is not primarily characterized by lack of appetite. The sufferer fights against hunger. Mara Selvini Palazzoli explains that “anorexia is not primarily a lack or a perversion of appetite, but an impulse to be thin, which is wanted and completely accepted by the sufferer”.4 The anorexia sufferer engages much of her energies in this constant fight against food, hunger and absorption of calories. The more she fights against food, the more food becomes important to her. Some anorexics are also vomiters. This condition is sometimes called ‘bulimic-anorexia’. People with anorexia sometimes binge, and like other people in a condition of malnutrition (prison or natural starvation), they constantly think of food.5 Food becomes an obsession. Their entire life rotates around food, food avoidance, choice of ‘safe’ foods, and ways in which ingested calories can be expelled.
People with anorexia and bulimia nervosa have a terror of fat and weight. Like all fears, this fear is dominating, and the person cannot find reassurance in others’ attempts to comfort. The experience of the sufferer, especially of the bulimic-anorexic, or of the bulimic, is to be trapped in a cycle that s/he cannot break. However, anorexia is not a condition that just ‘happens’ to the person. The urge to be thin and light is, in an important sense, deliberate. The sufferer willingly fights against hunger, and deliberately defends her eating and exercise habits. The sufferer thus plays an important part in the initiation and perpetration of eating disorders. This does not mean that sufferers should be ‘blamed’ for their condition – it rather means that, as they have the strength to fight against hunger, one of the most basic and compelling instincts, they also have the strength to adopt healthier lifestyles and to recover.
Bulimia nervosa
Bulimia etymologically means ‘ox-hunger’. Again, the term is inadequate to capture the drama that lies behind bulimia. The person with bulimia does not binge herself or himself because s/he is very hungry. S/he binges because of an urge, experienced as being out of control, to consume as much food as possible. The person will feel terrible about bingeing. S/he will feel dirty, guilty and above all profoundly ashamed. S/he will only be released from this anguish by getting rid of ingested food. The quickest way to achieve this is self-induced vomiting. Other practices aimed at getting rid of calories include use and abuse of laxatives and diuretics, self-induced vomiting, use of appetite suppressants and exercise.6
As neither starvation nor binge eating are caused by dysfunctions of appetite, the obvious questions then are: Why do sufferers starve? Why do they binge?
Eating disorders sufferers, whether anorexics or bulimics, are always overwhelmed with fears relating to body shape and weight, and invariably have a terror of fat. These fears – like any other fear – are experienced as being out of willful control. Consequently abnormal eating patterns are also experienced as being out of willful control. For this reason, as I will argue in later chapters, eating disorders have often been compared to addictions and other disorders of control of impulses (previously called obsessive-compulsive disorders). The person is obsessed with the fear of fat and with the thought of food and body weight. I will discuss various hypotheses on the causes of eating disorders in Chapters 3 to 5.
Binge eating disorder
Binge eating disorder refers to the condition of those who engage in food orgies of a bulimic type, but, differently from anorexia and bulimia, will not adopt compensatory behavior. At least some of the psychological dynamics involved in binge eating seem similar to those involved in bulimia. Eating is experienced as shameful and generates strong and sometimes unbearable feelings of guilt. However, people suffering from binge eating may tend to be overweight, whereas anorexics, bulimics or bulimic-anorexics might be underweight or have normal weight.7Therefore, the physiological characteristics of binge eating, including the secondary symptomatology that results from binge eating, are generally different to those typical of anorexia and bulimia.
Obesity
Obesity is defined as “a condition in which the natural energy reserve, stored in the fatty tissue of humans and other mammals, is increased to a point where it is associated with certain health conditions or increased mortality”.8 Obesity is defined and measured in various ways (see Chapter 6, ‘Globesity’).
Obesity may also be included among eating disorders in that it results from ‘disordered’ and self-destructive eating. Interestingly, whereas other eating disorders are classified as psychopathologies, obesity is not generally regarded as such, and is not included among psychiatric diseases. But what is the demarcation line between binge eating and obesity? What is it that makes binge eating a psychological or psychiatric condition, while obesity is not? Hilde Bruch,9 one of the first and still one of the most important scientists to have studied eating disorders extensively, in effect considered obesity an eating disorder. She showed that, in most cases, the causes of being overweight are psychological, not endocrinological or metabolic. This raises the issue of why some eating disorders are classified as mental illnesses, whereas other eating disorders (for instance, over-eating generally associated with obesity) are not.
This book is primarily concerned with anorexia and bulimia nervosa, both because these are most typically regarded as the ‘proper eating disorders’,10 and also because it is anorexia and bulimia that generate the most acute problems in the fitness and sports environment (see Chapter 6).
Anorexia athletica
The term ‘anorexia athletica’ was first used in the 1980s by Smith11 and Pugliese.12 It
Anorexia athletica is not a diagnostic category, and is not included in official diagnostic manuals.
In Chapter 6 I will return to anorexia athletica, to examine how the attempt to achieve excellence in sports and dance can trigger eating disorders. However, eating disorders and disordered exercise are not just problems for elite athletes or specific categories of professionals. They affect the population at large: young females mainly, but also older women and men and children.14 It is on the general population that this book shall focus. I shall discuss how exercise might represent a further threat for those already at risk, due to eating disorders, and the ethical dilemmas that exercise, connected with eating disorders, can pose to fitness professionals who work in the community.