- 224 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Case Studies in the Neuropsychology of Vision
About this book
One important means to understanding normal cognitive functions is the study of the breakdown of these functions following brain damage. This book provides reviews of major case studies dealing with the breakdown of visual perception and recognition, including the disorders of motion vision, colour vision, perceptual integration, perceptual classification, recognition of particular categories of object, semantic access from vision (in optic aphasia), and recognition impairments with relative sparing of imagery. The cases are discussed in the light of studies that have followed since, and the chapters provide a context in which the contributions of the case studies can be evaluated.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter One
Motion Blindness
Introduction
It is no longer disputed that one of the, albeit rare, consequences of brain damage is a remarkably selective impairment of vision. This contrasts with the scepticism that met earlier reports in the latter years of the last century of selective sparing, or disruption, of the ability to perceive motion or colour. Such disturbances were at odds with prevailing opinions about cortical organisation (see Zeki, 1990a, 1991, for reviews). The view was trenchantly held that the visual image on the retina, encoding the many attributes of the visual scene, was transmitted to, and passively analysed by, a single region of visual cortex residing in the occipital lobe. It was argued that if a single region were responsible for processing the many attributes of the visual scene then damage to this region should compromise the perception of all of them. Selective disturbance, or sparing, of a single attribute could not readily be explained in this scheme of things. Recent acceptance of the existence of selective disorders stems partly from substantial advances in our understanding, derived chiefly from animal studies, of the anatomy and physiology of the visual pathways in the brain. These studies have been supplemented by conclusions drawn from careful behavioural assessment of single neurological cases who have sustained brain damage.
The discovery of an impressive patchwork of cortical visual areas that lies in the extrastriate cortex of the monkey has led to the suggestion that each is relatively specialised for the processing of a particular visual attribute (see Chapter 2). The homologous, or analogous, regions in the human brain are now beginning to be identified and it is a simple step to conclude that the destruction of a single area will result in the disturbance of a single function. However, the problems with this apparently straightforward view are manifold (Cowey, 1994). First, some 30 areas have now been identified in the macaque monkey and we would perhaps be hard pressed to readily identify an equivalent number of visual attributes, e.g. colour, motion, form and depth. Certainly, one cannot easily infer the role of an individual area on the basis of the response properties of its neurons. The regional variation in receptive field properties of cells is not so clear as to provide an unerring indicator of the role of an area in visual processing. Second, only a small number of apparently selective disorders, e.g. impairments in the perception of colour, motion, form, space and depth, have, as yet, been identified in neurological patients. Third, and more alarmingly, surgical removal of a single visual area in the monkey has rarely, if ever, resulted in a deficit that parallels any of the clinical findings.
However, all is not lost. Selective disorders could reveal themselves in many guises and may not be revealed by tasks which merely require simple discriminations within a particular visual dimension. For example, impairments of colour memory, colour naming or colour constancy may exist without loss of colour discrimination (see Chapter 2). The difficulty may thus stem from establishing, and adequately specifying, the behavioural deficit. It is becoming clear that what can readily be viewed as a single visual dimension, e.g. orientation, direction, wavelength or disparity, can each be used to define a particular visual attribute. For example, a shape can be perceived, among other things, on the basis of chromatic, luminance or velocity differences between figure and ground. In principle, it is then possible for a deficit in the perception of form defined by one dimension to exist with a spared ability to perceive form defined by another. Such fractionation of disorders has become possible as perceptual tests become more sophisticated. Similarly, the fact that cortical areas cannot readily be distinguished on the basis of the proportion of cells responding to particular visual dimensions may reflect the crudity in the way in which receptive fields are characterised. The use of comparatively impoverished stimuli to test receptive field properties may conceal real differences among apparently similar populations. Thus, cells in area V1 respond to the direction of the component parts of a moving pattern while cells in area MT respond to the global pattern motion (Movshon, Adelson, Gizzi, & Newsome, 1985) and to the relative motion of a stimulus against its background (Allman, Miezin, & McGuinness, 1985).
Notwithstanding these difficulties, it is with one of the most striking disorders that considerable strides have been made in understanding its relation to the organisation and function of the primate visual system. The discovery of a region of the monkey brain, cortical area V5 (also known as MT), provided strong evidence that the visual cortex of the monkey brain is functionally specialised (Zeki, 1974). Neurones in this region are finely tuned to the direction of visual motion and it was promptly referred to as “the motion area”. Thereafter, the case of a patient with a relatively selective and profound deficit in the perception of visual motion was reported (Zihl, von Cramon, & Mai, 1983).
The Case of L.M.
In May 1980 a 43 year-old female patient, L.M., arrived at the Neuropsychological Unit of the Max-Planck-Institute for Psychiatry in Munich, Germany. She had sustained brain damage in October 1978 when she had suddenly lost consciousness and was admitted to hospital. L.M. reported that looking at objects in motion made her feel quite unwell. The explanation she gave sounded rather odd. She claimed that she no longer saw movement; objects which should move, as she well remembered, now appeared as “restless” or “jumping around”. Although she could see objects at different locations and distances, she was unable to find out what happened to them between these locations. She was sure that objects did not move, but appeared as “jumping from one position to the next, but nothing is in between”. Because of these difficulties she avoided streets, busy places, supermarkets and cafés. Traffic had become very frightening; she could still identify cars without any difficulty but could not tell whether they were moving or stationary. The only way for her to establish this was to wait until the car became either conspicuously bigger or smaller. However, this turned out to be very complicated, especially when there were other cars in the vicinity. As a consequence, she no longer risked crossing the street except at pedestrian crossings. When people walked nearby, she usually waited until they passed, because the “restlessness” they produced by their walking irritated her so much that she had to interrupt her walking to find a “resting point for my eyes”. Furthermore, she reported substantial difficulty in pouring fluids into a cup or glass, because the tea, coffee or orange juice appeared “frozen like a glacier”. She could not see the fluid rising, and therefore, couldn’t establish when to stop pouring. In addition, she felt very irritated when looking at people while they were speaking: their lips appear to “hop up and down”, so she had to look away so as not to become confused. “To my friends, this behavior appears very strange if not unkind; they believe that I am no longer interested in their conversation because I am always looking absent-minded. But it is the only way to listen to them without being disturbed”. For this reason she had decided no longer to meet her friends.
The patient quite accurately described her difficulties, and attributed them correctly to her illness. However, her difficulties were initially not assumed to be exclusively caused by brain damage, but were attributed, at least in part, to agoraphobia. The original diagnosis was made in the absence of any convincing alternative to explain her striking behaviour, especially in the first weeks and months, which presented a severe handicap in her daily activities. For example, she was unable to wash and dress herself, but had no obvious motor or somatosensory deficits; she had difficulty in understanding language, but had no aphasia; she could not perform activities like using a vacuum cleaner or preparing a plain meal, but had no apraxia. All her activities were extremely slow and cautious.
In contrast to these functional impairments, she seemed to have normal intellectual abilities, including memory and planning. Apparently no expert believed the patient’s report, probably partly because no similar case could be found in the neurological and neuropsychological literature. On the contrary, well-known authorities, such as Holmes, Critchley and later Teuber, had generally refused to accept clinical reports on selective impairments of individual visual functions (for a detailed review, see Zeki, 1993). Admittedly, in contrast to the body of evidence for the existence of achromatopsia, the selective loss of colour vision (Zeki, 1990a), the evidence for selectively impaired movement vision was not strong before the report of patient L.M. (Zeki, 1991). The only case with impaired movement vision after acquired brain damage that had been examined in detail was reported by Goldstein and Gelb (1918) (case Schn …). However, these authors interpreted their case as a special type of apperceptive visual agnosia (“visual form agnosia”). Accordingly, Goldstein and Gelb considered the loss of movement vision in the same patient as just one symptom of the impairment in (actively) constructing a Gestalt. Poppelreuter (1923) doubted the “pureness” and specificity of visual form agnosia in this case, because the patient showed additional visual deficits, among them a concentric loss of form vision in the region of the extrafoveal visual field, which could explain his difficulties with the identification of moving visual objects. In addition, Jung, who in 1949 published a detailed re-examination on the same patient, put the existence of visual agnosia in this case in doubt, because he was unable to find evidence for a “form or movement blindness”. Jung recognised the scientific value of singlecase studies, but stressed the importance of “elaborated” examinations in such studies. This view was later adopted by Shallice (1977), who pointed out that detailed experimental analysis of single cases can sometimes contribute much more to the understanding of brain organisation than group studies of patients with multiple defects which are difficult to compare. This argument is particularly forceful since cases with selective functional deficits caused by brain damage are extremely rare. No doubt this is because, as Campbell pointed out at the beginning of the century (1905), “… it is almost impossible for nature to restrict a damaging lesion to the cortex, and to the cortex only, in question.”
Behavioural Consequences of L.M.’s Movement Vision Disorder
When L.M. was first tested, some 18 months after brain damage had occurred, she was severely handicapped. At that time she lived alone because her husband had died about three years earlier. Before her illness, she had been running a small electrical retail business. Although she showed considerable improvement during her stay in the rehabilitation centre, she was judged as totally disabled in her daily life. In August 1980, Dr Mai and one of us (J.Z.) provided regular practice for L.M. with daily activities like crossing streets, using buses and the tube, shopping in supermarkets, walking in the presence of other pedestrians, cooking, cleaning the apartment, active participation in discussions (starting with only two people), and writing. Of course, understandably L.M. was often very frightened and developed an exaggerated caution, and sometimes showed clear symptoms of distress. The “treatment” lasted for about three years, but since then L.M. copes quite well with her difficulties. She has adjusted successfully to the demands of daily life, lives independently in her own apartment, and has an active social life. She has become proficient at avoiding distressing situations but is nevertheless better at coping with them. Accordingly, she organises her daily activities such that she arranges shopping when the supermarket is nearly empty, uses public transport outside rush hours, and never invites more than four people at once to have tea or coffee with her. Of course, her friends are acquainted with her problem and understand the peculiar nature of her behaviour in certain situations.
Despite L.M.’s very efficient adaptation, the degree of the impairment of her movement vision has not changed essentially (Zihl, von Cramer, Mai, & Schmid, 1991). She still shows severe impairments in conditions where she would need the ability to see movement. For example she still has difficulty in guiding her moving hand visually. Figure 1.1 shows an example. When L.M. was asked to write a word with her eyes closed, she performed much better and faster than when asked to write the same word with her eyes open. In the latter condition she had to stop several times because “my fingers and my hand are somehow restless, and this disturbs me.” A similar problem exists with walking; L.M. tries to avoid looking at her feet because their movements would distract her. In town she feels safe when walking along the walls of houses; otherwise she is unsure if an approaching person is likely to collide with her. “Sometimes I do not even know whether a person is approaching me or is receding.” When using the bus or tube, she avoids looking out of the window.
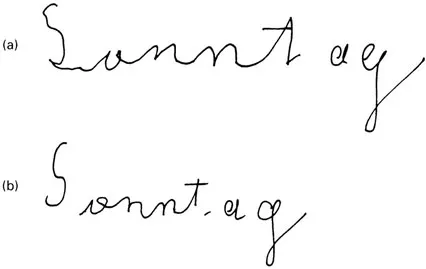
Fig. 1.1 L.M. was asked to write “Sonntag” (a) with eyes open and (b) with eyes dosed. She was substantially less hesitant with her eyes closed, reflected in the time taken to perform the task: eyes open, 26s; eyes closed 4s.
Moving stimuli persist in being highly disturbing and unpleasant to L.M. Even after countless hours of testing and intensive practice with moving displays, she finds the experience uncomfortable. Regular breaks are required to avoid such discomfort as much as possible. Usually, after about 30min of testing, she no longer looks at moving stimuli and experiences a strong feeling of nausea and unpleasantness which she has difficulty in describing. She would comment “To me, everything becomes restless, and so I have no idea where to look at and what to do to find out which response would be the correct one.” This experience, which has not essentially changed over the past 15 years, is in clear contrast to patients with achromatopsia, who report their surroundings as “pale” or “drained of colour”, but the absence of colours does not seem to cause similar discomfort.
Neuropsychological Assessment
L.M. had been admitted into hospital in a state of stupor on the 7 October 1978. Examination did not reveal any focal neurological symptoms. On panarteriography the cortical veins in the temporoparietal region were not filled, and a superior sagittal sinus thrombosis was diagnosed. In the next weeks the patient’s health status improved considerably, and she could eventually be transferred to a rehabilitation centre. There, she undertook systematic regular practice with daily activities and was, in addition, treated for agoraphobia.
When L.M. was first seen by one of us (J.Z.) in May 1980, about 19 months had elapsed since her admission. She still showed general slowing and tended to fatigue easily; after about 20–30min of testing she felt exhausted. Detailed neurological and neuropsychological examination did not reveal any motor or somatosensory deficits. No apraxic symptoms were present. Verbal and nonverbal memory performance was in the lower normal range; topographical memory was normal. She showed mild anomia which involved all modalities equally. She had difficulties in copying and drawing from memory (Grüsser & Landis, 1991, pp. 372–3) and with writing. When asked for an explanation for these difficulties, she complained that she felt disturbed by tracking the trajectory of her own right hand. This visuomotor disturbance was more or less unchanged even ten years later (Rizzo, Navrot, & Zihl, 1995). Visual fields were full for light, colour and form targets, and there were no signs of visual neglect or impaired simultaneous vision. Visual acuity, spatial and temporal contrast sensitivity, colour vision, discrimination of greys and fo...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright
- Contents
- List of contributors
- General background
- 1. Motion blindness
- 2. Cerebral achromatopsia
- 3. Integrative agnosia
- 4. Apperceptive agnosia: A deficit of perceptual categorisation of objects
- 5. Vision and visual mental imagery
- 6. Category-specific recognition impairments for living and nonliving things
- 7. Optic aphasia: A review of some classic cases
- 8. Covert recognition and anosognosia in prosopagnosic patients
- 9. Relations among the agnosias
- Author index
- Subject index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Case Studies in the Neuropsychology of Vision by Glyn W. Humphreys in PDF and/or ePUB format, as well as other popular books in Psychology & Cognitive Neuroscience & Neuropsychology. We have over 1.5 million books available in our catalogue for you to explore.