- 236 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
A classic book on the use of expressive therapies with uncommunicative elders and the disabled. This poignant guide explores group and individual therapeutic activities that promote creativity, self-expression, communication, and understanding of one's life. An experienced art therapist relates his insights into the psychosocial dynamics of elders and the disabled and shares his awareness of the sensitivity and understanding required to reach the "unreachable." Health care workers will find this illustrated volume rich in therapeutic techniques and processes applicable to the care and growth of psychologically and physically disabled or minimally handicapped adults and elders.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Section I:
Expressive Therapy Techniques and Case Studies
Chapter 1
Regression of the Hospitalized Elderly and Disabled Patient as Explored Through Art Therapy
PART I
Regression is an emotional, behavioral, and cognitive enactment of a return to a previous time in a person's life. People who are regressed often relive, in a compulsive manner, desires, feelings, thoughts, and actions from their past. Regression can be caused by organic problems (e.g., stroke, Korsakoff ‘s syndrome), or may be induced by psychological problems (e.g., traumatic experiences, lack of nurturing), or by an impoverished environment. Regression can act as a maladaptive action in avoidance and denial of the present reality, or as an ego-sustaining activity in a physically, emotionally, and psychologically painful situation. This chapter will focus on the psychological causes and effects of regression and how this process is explored through art therapy.
The phenomenon of regression in institutional settings is often a major problem. Elderly and disabled people who live in institutions or hospitals often experience a loss of self-esteem, self-assurance, and integrity due to the loss of their independence and self-reliance, and a loss of significant relationships. These feelings of loss can induce withdrawn and isolative behavior which acts as a catalyst for further regression.
Frustration of wishes and needs produce conflict and stress, which are the basic elements of neurosis; but the successful resolution of conflict is the basis of growth and development.1
Elderly and disabled individuals often have few opportunities for the resolution of personal conflicts within the institutional setting; therefore, maladaptive patterns of dealing with conflict and stress may appear, such as, withdrawal, isolation, and regression. These patterns of behavior are often seen in their nonverbal expressions.
A way of dealing with conflict and stress for regressed patients is seen in the nonverbal messages they give by clinging to their beds, blankets, pillows, or other people as they seek a means to express their need for consistency, validation, and relationship with others. Through holding onto and fixating upon certain types of behavior, patients are able to control, to a certain extent, the stimulus from their environment, helping them to feel a sense of self and personal power.
During my work as an expressive therapist at a long-term care/ rehabilitative facility, I was able to perceive the regressional processes caused by organic impairments, psychological conflicts, and by the patients' social situations. Thus, the following therapeutic approach was structured to compensate for the tendencies of patients to regress and isolate.
I found that a patient's regressional process may be significantly lessened through a stimulating, nurturing, communicative, and interactive environment. The group art therapy experience gave patients a chance to express their feelings, thoughts, and concerns, and be recognized by themselves, their peers, and staff in an activity which counteracted the patients' regressional tendencies. Through this process, patients began to feel and act as individuals, expressing their feelings and thoughts, feeling proud of their activities and of themselves. They found that just being aware of and in communion with others gave significance to their lives.
The art therapy group consisted of from five to fifteen elderly and disabled participants, and was held at a round table in the day room. The sessions would begin by handing out art materials, putting on some lively music, and talking to the group about a theme they could explore through writing, drawing, or painting, individually or together. Patients were encouraged to share their feelings and thoughts with each other in order to bridge their isolation and develop a sense of community.
An important aspect of the art therapy process was for patients to uncover and discuss various personal, conflictual, and timely issues during the group activity. The recognition of the individuality and importance of each person is essential to the integrity of this process. Without this recognition, patients may begin to regress and isolate.
During the art therapy sessions described in the following pages (the cases of Mr. K, Mr. H, and Mr. B), aspects of the patients' regressional processes became apparent, and significant issues and concerns were brought up and addressed. By the aid of the art therapy process a sense of community, intimacy, personal recognition, and sharing was created within the group setting.
The Regressional Process as Noted with the Severely Handicapped-Regressed Patient.
In group art therapy sessions, I noticed that each person usually drew only within a small area in front of himself. However, the very confused patient would often draw outside this confined space because of difficulty in perceiving boundaries. Mr. K, a participant in the art therapy group, was a confused patient in his sixties whose medical diagnosis was senile dementia. In art therapy sessions which were focused on group murals he would scribble over other patients' writings and drawings as if he did not notice them (see Photo 1.1). He also scribbled randomly on any nearby object. His art activity could be compared to the description of a child's art expression in Rhoda Kellogg's book, Analyzing Children's Art:“The Emergent Diagrams do not rely on the edges of the paper for definition, nor do they present clear shapes. “2 This lack of boundary and image clarification is often characteristic of the very confused patient (see Photo 1.2).
In Mr. K's drawing style and picture (as with other regressed patients), a regression and fixation to childlike behavior is evident. His drawing style was comparable to that of the early stage of childhood in which children draw circular patterns by means of long arm movements. At this stage, children also produce sounds with the crayon or the art tool as an exploratory and sensory stimulus during the art activity. While he drew, Mr. K often made tapping noises with his felt-tip pen or crayon, feeling the texture of the paper, engrossed in the drawing experience. Mr. K was usually so involved in the task of drawing that he did not notice the people around him or the boundaries of the paper.
Mr. K's responses in art therapy typified his exploration of his surroundings in a “regressive” tactile and sensory mode; touching, tapping, and drawing on whatever was in reach. His art expression was his way to relate to the world in a manner that he could experience and feel acknowledged.
PHOTO 1.1. Group mural. Mr. K's drawing of random scribbles (long continuous lines) is located at the top of the mural. Mr. B's drawing (circles and dots) is at the top left of the mural. Notice that Mr. K drew over Mr. B's picture.
PHOTO 1.2. Mr. K's painting. Notice the lack of clear shapes and forms.
The Regressional Process as Noted with the Moderately Handicapped-Regressed Patient.
The symptoms of moderately handicapped-regressed patients may appear as a reflection of their uneasy feelings and thoughts toward their situation which they would like to deny, avoid, and forget. Patients often have much difficulty verbalizing these uneasy feelings and thoughts. Through the use of art therapy such feelings can be brought out in a nonverbal, nonthreatening manner and discussed openly.
I found that regressed elderly and disabled patients in the art therapy group who were not severely confused or disoriented displayed a need to control their environment. They rarely reached out to others, typifying the isolation found with these populations. The act of setting boundaries in their art expression is shown by a regimented style of drawing as seen on a representative group mural (see Photo 1.3). This confined drawing style, where each patient drew only within an enclosed area, symbolized their need for order and control. These patients would set increasingly rigid boundaries in their interactions and movements, as well as in their drawings.
Mr. H, a mildly regressed patient in his seventies, joined the weekly art therapy group. He was diagnosed by the doctor as having a mild case of senile dementia with schizoid tendencies. Mr. H had an obsessional craving for food, his bed, and companionship. At the beginning of the art therapy sessions he would sit stoically and silently, but after a few minutes of silence he usually blurted out a request in a loud, demanding, angry, almost pleading tone of voice, as if speaking to people who were ignoring him. He usually asked to either go back to his bed or to have something to eat.
In one of Mr. H's first art therapy sessions he drew expressionless faces with wandering eyes and no mouth (see Photo 1.4). This picture resembled, in an abstract way, two nurses and a staff doctor who worked on his ward. During a discussion of the drawing with Mr. H, I realized that his picture represented the feelings he often expressed about the staff. He felt the staff gave a seemingly empty display of concern for him and desire to help him. Whenever he mentioned this feeling he seemed to become quieter and more withdrawn. After he drew a picture in the art therapy session he would usually sit back and ponder it, looking more relaxed and at peace with himself. I felt at these times, through his art and writing, he had made a significant statement to himself, or acknowledged his feelings and felt recognized.
PHOTO 1.3. Group mural done by four patients. Notice that each person keeps to his own confined area, and there is no graphic interaction.
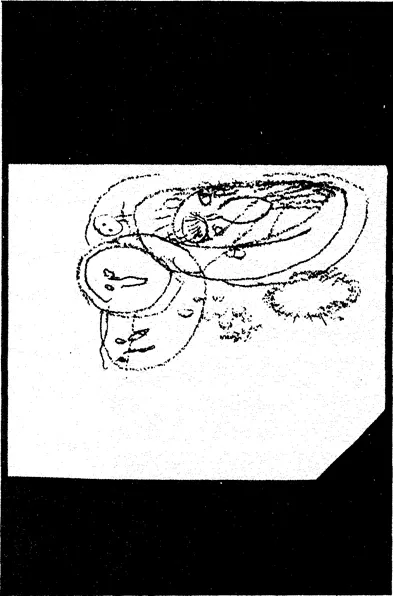
PHOTO 1.4. Mr. H's drawing which resembles faces of two nurses and a doctor who work on his ward.
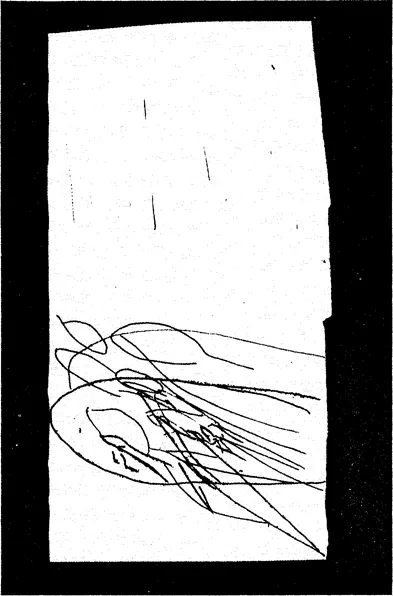
PHOTO 1.5. Mr. H's drawing using random marks producing an unclear image.
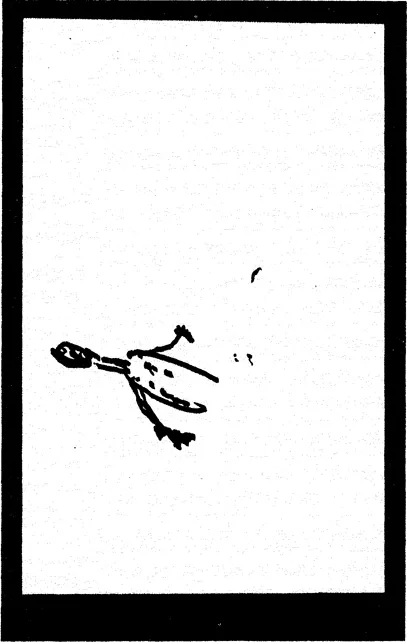
PHOTO 1.6. Mr. H's drawing of what he called a “blank man.”
Mr. H often told me that he was lonely in the hospital. His obsessional demands could be seen as a regression to childlike behavior and as an attention-seeking request for nurturing, compassion, and relationship with others. The demands were primarily oral and tactile (as noted by his requests for food and touching) which are common with regressed patients. His requests signified a number of possible factors: the lack of sensory stimulus in the institutional setting, his feelings of isolation, loneliness, withdrawal, and unmet needs. Mr. H's behavior exemplified the tendency in patients to isolate due to their anger and frustration, thus reinforcing their regressional process. This process may also manifest as an obsessional craving for physical comfort, food, and caring.
At the next art therapy session, Mr. H drew a picture of lines in random order with no structure or theme (see Photo 1.5). When I asked him what he was drawing he exclaimed in a loud sharp voice, over and over, “This is nothing, nothing.” At the end of the session he was in an angry, silent mood and wheeled his wheelchair into the ward, next to his bed. Later in the day, when he was in bed, I asked him how he was feeling. He replied in an angry tone, “I want to go home!” I said, “Isn't this your home?” He replied in an even angrier and louder voice, “What do you think, the way they treat me!” His words bit at my bones and I felt his pain and anguish.
Mr. H's anger was reflected in the way he acted, particularly in his obsessional pleading for favors. This was compo...
Table of contents
- Cover
- Half Title
- About the Author
- Full Title
- Copyright
- Dedication
- Contents
- EDITOR
- Acknowledgments
- Preface
- Foreword
- Introduction
- SECTION I: EXPRESSIVE THERAPY TECHNIQUES AND CASE STUDIES
- SECTION II: THE EXPERIENTIAL PROCESS
- SECTION III: THE CONCEPTUAL FRAMEWORK
- Conclusion
- Appendix: Charting the Creative Arts Therapy Experience
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Expressive Therapy With Elders and the Disabled by Jules C Weiss in PDF and/or ePUB format, as well as other popular books in Psychology & Developmental Psychology. We have over 1.5 million books available in our catalogue for you to explore.