eBook - ePub
Eating Disorders: Time For Change
Plans, Strategies, and Worksheets
- 188 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
This collection for therapists and clients presents practical, how-to information, for the treatment of eating disorders. The authors have kept the needs of the therapist in mind by considering managed care as well as specific therapeutic issues. This resource will maximize the efficient use of time and resources for the therapist and increase the efficacy of work with clients with eating disorders. Clients will find the tools to be helpful resources and a critical extension of individual therapy.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Subtopic
Mental Health in PsychologyIndex
PsychologyCHAPTER
1
Introduction
In eating disorders treatment, frustration often reigns among clinicians. We see immense suffering and are unable to ameliorate it. We see clients not making progress in outpatient treatment sessions and, although progress may be made in inpatient and partial hospital settings, often it is lost upon discharge. We witness the revolving door of clients going in and out of treatment facilities without recovery. We see clients in what appears to be interminable outpatient care only to observe the chronic course of illness setting in. At other times we see clients, against all odds, turning their lives around. We see long courses of suffering melting, finally, into the sweetness of recovery. We see clients on their third, fourth, and fifth hospitalizations, finally breaking free of the bonds of illness. Or we see the client who has given up hope suddenly finding meaning in her life and freeing herself from starvation, bingeing, and purging. When we are truly fortunate, we see our clients valuing their lives, finding their voices, and breaking free of self-destructive behaviors and ways of thinking even when others cannot applaud their progress.
What is it that assists one client in her efforts toward recovery, but seems not to move another? What is it that helps one client eat … but pushes another into more intense starvation (often when out of our view)?
We believe it is, in part, serendipity. If we fall upon the right intervention, the right word, the right metaphor, the right strategy, the right structure for the right or opportune moment in a client's life, then we may view, with great awe, the epiphany … the awakening of a life. But if we implement the same strategy, intervention, word, or metaphor at another moment in the client's treatment, we may overwhelm, hurt, or discourage the client in her pursuit of help.
Our timing, tone, words, and approach can determine how effective or ineffective is our intervention.
We have often observed that people with eating disorders need control. Perhaps it is that they, more than most, are unwilling or unable to grant control to others who go against their very nature, timing or appetite. It may be that progress is not seen in the numbers one would expect because clients are being pushed or coerced into a course of treatment that is not of their making. The exception to this rule, however, applies to clients who are medically or psychiatrically at risk. Medical and psychiatric interventions must occur to prolong or save a life, even when the client is precomtemplative and unable or unwilling to recognize the problem or act to save her life. But it is the rare client who indeed meets these criteria of imminent risk. We are now speaking of the majority of clients who feel treatment is either ineffective or, at times, detrimental because the course or content of the treatment does not meet the client where she is.
How can we match the treatment to the client? How can we ensure better, long-lasting outcomes?
We believe the answer is in understanding the stages of change thoroughly researched and scientifically proven by Prochaska and colleagues (Prochaska, Norcross, & DiClemente, 1994]. Matching the intervention to the stage of change of the client and working within that stage will help the client move to the next stage. It is the need to trust that the matching and mirroring of the client's timing, or stage, with our intervention, will yield more positive and long-lasting results than the following of a course of treatment that meets some other need, not that of the client.
Although many clinicians are intuitively in touch with their clients’ needs, most of us do better by our clients if we are following a structure. Our task is to teach about these stages of change, match the appropriate stage intervention to the client, and move sequentially through the stages with the client. It is, in many ways, like knowing what normal development is for a child, and supporting the child at each step consistent with what that child needs at each step. When we are out of step, or not matching the intervention to the stage of change of our clients we may either be unhelpful or potentially hurtful. When our interventions are timed appropriately, we further the process of development and progress. As an example, when we do not provide a 2-year-old child with the safety and security of our presence, that child might not go off to explore, which is developmentally appropriate. But, when that child feels secure, she will explore readily because she does not have to worry that we'll be there when she is done.
It is our task to provide the safety, security, information, and plan of intervention that will foster each client's efforts at growing the competence and confidence that she can manage her feelings and the world without the eating disorder. This is more likely to occur if we meet the client at her stage of change.
James Prochaska and his colleagues, John Norcross and Carlo DiClemente, set out to understand why some people–those who do and do not seek professional help–either succeed in changing unwanted and problematic behaviors, or do not.
What they found was that most treatment programs, for a large number of problematic behaviors, meet people at the “action” stage of change, yet less than 20% of people who seek treatment are actually at that stage of change. Therefore, excellent programs often fail … not because they are not good, but because they are good only for the small segment of the population that is ready to change now.
Consequently, many clients blame themselves, the therapist, or facility for no progress. Some leave treatment or experience diminished self-esteem due to the perception that all they do is fail. Many therapists and facilities reinforce this belief by blaming the patient and impugning her motivation.
In Stages of Change theory, it is known, accepted, and understood that most clients who are in treatment, are not ready for change at the action stage. Yet, they may be ready for an intervention at an earlier stage of change.
THE STAGES OF CHANGE
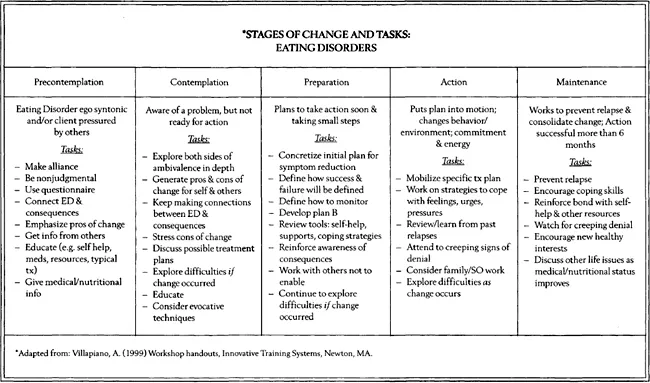
According to Prochaska etal. (1994), there are six stages of change: 1) Precontemplation, 2) Contemplation, 3) Preparation, 4) Action, 5) Maintenance, and 6) Termination. These stages are predictable, follow for all people no matter what problematic behavior they want to change, and are of equal importance in the change process. They have found that matching the intervention to the client's stage of change yields better results than imposing an intervention that does not match the client's stage of change.
We will briefly describe the stages and give examples of stage-appropriate interventions.
Stage 1: Precontemplation
In the Precontemplation stage, the client does not want to be in therapy; she is there under duress. She does not see the symptomatic behaviors as undesirable, or she wishes to maintain the behaviors. Is this not how many clients enter therapy? Many are children who are not allowed to resist therapy. Physicians tell others that they will be hospitalized if they are unable to turn their eating-disordered behavior around. Often, school personnel or employers tell clients that symptomatic behaviors or physical conditions will interfere with their involvement unless something is done.
In cases like these, education and an emphasis on the pros of change is most effective. Surprisingly, many clients are not educated about their illness and the ramifications of continuing on the same course. They are not given the reasons, concrete and factual, why change is good. These are the clients who, if hospitalized or placed in treatment against their will, will likely go through the motions of change, but revert to old behaviors once discharged or out of the sight of therapists or loved ones.
Stage 2: Contemplation
A client in the Contemplation stage is one who understands the pros of change, but must mourn the loss of the symptoms … and thus, the illness. With this client, time must be taken to look at the cons, as well as the pros, of change. How will her life change for the worse? What will she have to give up, do, or feel without this illness? A thorough exploration of these issues and feelings leads to an acceptance of the eating disorder's loss and a moving on.
In treatment, this stage is often overlooked. It is difficult to help a client explore and express reasons why the illness has been good for her, when we see it as nothing but destructive. Yet overlooking the needs of the client at this stage, in an effort to push her into action, often backfires and the client holds more stubbornly to the symptoms that keep her safe.
A young woman and former client, upon trying to understand what led to her recovery after years of severe illness, simply stated, “patience” … the patience of her therapist … which may have led to her eventual readiness to move to the next stage of the change process. Working with clients … patiently and compassionately … at whatever stage they present, works. Forcing clients into premature action does not.
Stage 3: Preparation
The client in the Preparation stage needs help and rehearsal in preparation for action. This is the stage when the client and therapist identify the goals of behavior change and strategies to reach those goals. This is where they prepare their “war plans” … how they will attack and subdue out-of-control behaviors and thinking patterns. This is where they work to secure their environment and bring in as many supports as possible to fortify their efforts.
Most clinicians do well in this stage, but may make the error of pushing action before the plan is fully in place and the client is fully prepared for battle. As in all famous and successful historical battles, foolproof plans secured victory, not impetuous action.
Stage 4: Action
In most treatments and treatment facilities, clinical staff are perched for action. Clients are propelled into action when many are not ready to act. For those who are in the Action stage, the treatment is effective and changing for the good occurs. For those who are not, time and money is wasted, and hope is thwarted.
Action is doing that for which the client is ready and prepared. Action is the active changing of symptomatic behaviors and the trying-on of new, more adaptive behaviors. It is the stage of change that we most value, but as Prochaska and colleagues state, it is no more important in the quest of “Changing for Good” than any other stage. All are important and all must be addressed for successful, long-term change to occur.
Stage 5: Maintenance
In this stage, practice, practice, practice, is the key. Clients need reinforcement to maintain new behaviors and ways of thinking. Usually, the Maintenance stage is one of intense struggle and growing confidence. Here clients will solidify change.
Stage 6: Termination
Clients in this stage have mastered the change. This is when most clients no longer need treatment. They have internalized the skills to maintain the change.
Usually, clients who present for treatment do so in one of the first four stages. We will focus our book on treatment approaches and interventions that are most effective with clients who present in precontemplation, contemplation, preparation, action, and maintenance. We will talk little about the Termination stage, as we, like our primary care physician colleagues, believe that as mental health professionals we must be available to our clients throughout the lifecycle. Although they may no longer need our care for the eating disorder, they need to know we will be available to consult with them should other issues arise in their lives.
We have also seen that our clients may be in different stages of change for different symptomatic behaviors or problems. Matching the intervention to the stage for each symptom or problem will increase the effectiveness of the treatment. For example, a client may not want to change her weight, but she may be ready to stop purging behaviors. We would address these problems with different interventions appropriate to the client's stages of change.
It is our task to present a plan and approach to the treatment of clients with eating disorders, that neither ignores medical and psychiatric sequellae, nor the press of time, while still honoring the client and matching the treatment to her stage of change. Ultimately, matching the intervention to the client's stage of change minimizes the occurrence of medical and psychiatric crises, takes less time over the course of the illness, respects and affirms the patient and her needs, and leads to Changing for Good.
The following chart depicts how the stages of change can be applied to the treatment of eating disorders. Under each stage are a list of tasks to accomplish at each stage. Use this chart as a template for determining how to work on eating disorder symptomatology at each stage. The various chapters will go into the tasks associated with each stage in greater detail, especially as they relate to clients’ unique situations.
SUMMARY
In this chapter, we reviewed the Stages of Change theory (Prochaska et al., 1994). We looked at some examples of how to apply this theory to our work with clients with eating disorders. If you have worked with clients with eating disorders before, you know that your clients present as unique people with unique problems. Stages of Change theory provides a template for understanding the unique needs of your client so you and she can formulate a plan for change. We have found that our clients engage in the treatment more readily if they have an opportunity to identify their own stages of change. It seems to help them feel more partnership in the process and it fosters intrigue and engagement in the tasks at hand. Perhaps, most importantly, however, this theoretical approach fosters a gentle and patient approach to the client who is not at all ready for change (one in precontemplation stage) as much as it encourages an energetic, action-oriented, problem-solving approach to the client who is ready to change now (action stage). It can soften the harsh judgement of the client against herself (because she is not ready to change now), and it can remind all of us that, in general, our clients are doing the best they can.
The next chapter, Therapist Issues, is meant to encourage those of you who work with clients with eating disorders to reflect upon the issues our clients have raised with us. It also provides questions to ask yourself if you are contemplating working with clients with eating disorders.
The following chapter deals with assessment, and includes self-report forms for the client, family, and significant other. The chapters thereafter deal with issues of: hunger, restrictive eating, binge eating, purging, body image and weight, athletics, substance abuse, and sexual abuse. The final chapters focus on nutritional counseling, medical care, and psychopharmacological issues and management.
In order to protect the confidentiality of our clients, we do not use their real names in the personal vignettes you will read. Much of the identifying data has been changed, as well. Though these changes result in fictional accounts, the feelings, issues, needs, tragedies, and triumphs of these clients are real.
CHAPTER
2
Therapist Issues
Goals:
Table of contents
- Front Cover
- Half Title
- Title Page
- Copyright
- Dedication
- Contents
- Acknowledgments
- Preface
- Chapter 1 Introduction
- Chapter 2 Therapist Issues
- Chapter 3 The Initial Assessment
- Chapter 4 Understanding Hunger
- Chapter 5 Food: Fear and Restriction
- Chapter 6 Binge Eating and Purging
- Chapter 7 Body Image and Weight
- Chapter 8 The Athlete
- Chapter 9 Substance Abuse and Eating Disorders
- Chapter 10 Sexual Abuse and Eating Disorders
- Chapter 11 Nutritional Counseling
- Chapter 12 Medical Care
- Chapter 13 Psychopharmacological Issues and Management
- References
- Recommended Reading
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Eating Disorders: Time For Change by Mona Villapiano,Laura J. Goodman in PDF and/or ePUB format, as well as other popular books in Psychology & Mental Health in Psychology. We have over 1.5 million books available in our catalogue for you to explore.