![]()
Part I
Learning How to be a Professional
In this part the decision-making process in speech and language therapy assessment and management is outlined and the skills required in order to work in professional practice are discussed. It is recommended that Chapters 1 and 2 are read together. The reader will be guided through the issues relating to professional development, the first job and the learning process of the developing speech and language therapist. A speech and language therapy manager highlights in Chapter 3 important areas of consideration when applying for a first job.
![]()
Chapter 1
The Decision-Making Process in Speech and Language Therapy
Myra Kersner
Learning Outcomes
By the end of this chapter, the reader should:
have knowledge of the speech and language therapy decision-making process when working with children;
have knowledge of the choices available and how speech and language therapists make decisions in their work;
have knowledge of the speech and language therapy management process.
Introduction
The management process in speech and language therapy begins as soon as children are referred and therapists need to make decisions about how to proceed. Initially these relate to the choice of assessment procedures and whether or not intervention is required. Then, choices will have to be made about the best approach to therapy. Further assessment decisions will be made, if appropriate, throughout the process resulting in options for review and discharge.
The management process can be divided into four major stages:
forming working hypotheses;
assessment, including information gathering, observing and interpreting behaviour;
setting objectives for therapy;
facilitating and evaluating change.
Any process comprises a series of actions occurring over time. Processes are organic, each aspect affecting and being affected by other aspects. Within the process there is fluidity of movement until an agreed end point and a desired outcome is eventually achieved. In speech and language therapy each decision within the process will affect, and be affected by other decisions as well as being influenced by the specific setting, the individual child and the context.
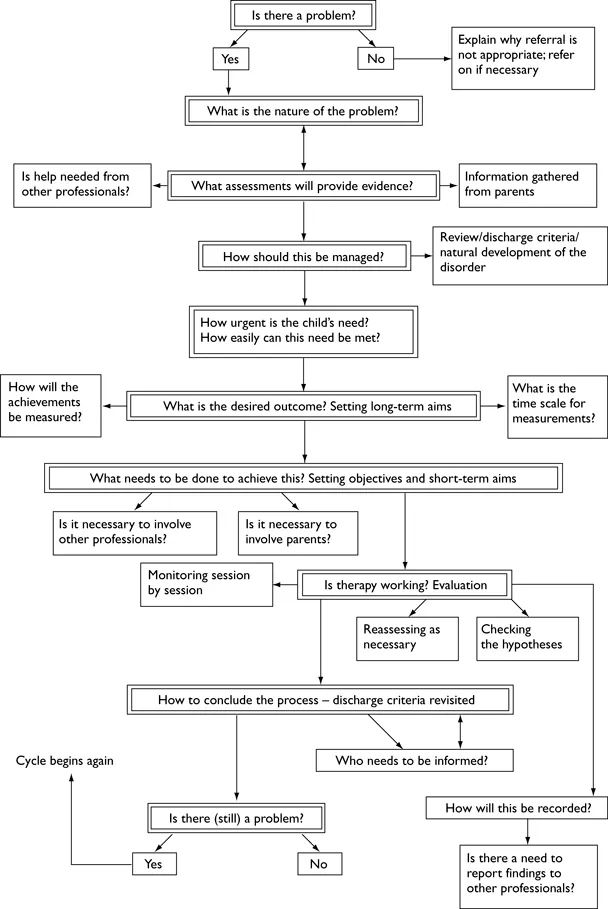
Figure 1.1 offers a framework in which the management process may be considered in terms of the decisions which need to be made. For different ways of representing the process see for example Bray and Todd (2005) and McAllister and Lincoln (2004). Although the decisions appear in linear order, it is in fact a cyclical process (see also Figure 2.1, Chapter 2) so that the sequence in which the decisions need to be made is not fixed. Some may be bypassed while others may need to be made simultaneously.
Figure 1.1 The decision-making process.
In this chapter there will be discussion about the types of decisions which need to be made within this framework, the overall choices available, the questions which need to be asked and the ways in which speech and language therapists approach the process as a whole. For specific decisions that relate to the nature of the setting in which the child is seen see Chapters 4–7; decisions made in relation to specific disorders will be discussed in Chapters 10–22.
The Decision-Making Process
The Time Period
The time in which individual decisions have to be made is normally governed by the context and the setting. In some instances, assessment and decision-making regarding future management may occur at the initial meeting. In a Child Development Centre, for example, the focus may be on multi-disciplinary assessment, and the children may only be seen once, or for a limited period, before being referred to other centres for therapy. However, when working with children in schools, the information may be gathered over a longer period and assessment-therapy reassessment may be part of an ongoing ‘diagnostic therapy’ process.
The length of time required for improvement or change to occur may vary greatly and, while some children will achieve their goals within a fixed-length block of therapy, others may require help and support over a protracted time.
A Child is Referred
Is There a Problem?
Decision: Yes/No
The management of a child with speech, language and communication needs (SLCN) begins on receipt of the referral. The therapist forms an initial working hypothesis about whether or not a problem exists, what might be the nature of the problem and what to do about it.
Case Example: Sophie
Kate, a speech and language therapist, receives a referral letter from a nursery school teacher describing Sophie aged 3;2 as having ‘unintelligible speech’. Kate will have to draw on her professional knowledge to help specify the nature of the problem, identify possible contributing factors and to establish whether such a problem may be dealt with appropriately by a speech and language therapist.
The first question to be asked is whether or not the problem actually exists. There are three reasons why this is important.
The referral may have come from a concerned teacher, or a conscientious health visitor, but the parents may not consider there is a problem.
The parents may believe their child has a communication problem but the teachers or medical personnel may not agree.
The child may once have had a problem, but have improved spontaneously so that it no longer exists.
If Kate decides Sophie’s communication does not require intervention, she will need to explain this, with her reasons, to the referrer.
It may not always be easy to discern whether or not a problem exists. For example, at initial interview some children may be unwilling to speak. Children often perform differently when faced with an unknown adult, than when interacting with a group of their peers. Some children have high level language difficulties which may not be apparent on first meeting. Or, a child who has been referred because of a stammering difficulty may speak fluently to the therapist at initial interview.
In order to make the decision about whether Sophie’s problem exists, Kate must gather supporting evidence from a variety of sources, such as focused observations of Sophie’s play and interactions with others, which can then be compared with the norms for her age and developmental stage. Kate will also ask Sophie’s parents preliminary questions, talk to her nursery teacher and look at any previous records.
It may be that Kate’s decision is ‘no’, this is not a problem for the speech and language therapist. She also needs to consider whether Sophie has a problem that would be more appropriately dealt with by someone else. For example, if she seems to be developing slowly in all areas she may need to be referred to a paediatrician or a psychologist, with an appropriate report.
If Kate’s decision is ‘yes’, Sophie has a communication problem, then working hypotheses will need to be developed and tested.
What is the Nature of the Problem?
Decision/Question: What are Kate’s Working Hypotheses?
In order to develop her hypotheses Kate will need to gather more detailed information. This will include assessing Sophie’s comprehension of language, recording and transcribing a detailed speech sample and/or a language sample, using appropriate informal and formal assessment procedures (Lees and Urwin 1997). Kate will now ask more detailed and appropriately targeted questions of Sophie’s parents and her nursery teacher to establish Sophie’s communication patterns in a variety of contexts and settings. As Kate puts together pieces of the puzzle she will form new hypotheses which can be tested and accepted or rejected until she has an accurate, holistic picture of Sophie’s communication skills. This should then indicate a possible approach to therapy.
What Assessments will Provide Appropriate Evidence to Support or Refute the Hypotheses?
Decision/Question: What are the Criteria for Choosing or Rejecting Assessments?
What are the choices available? No child should routinely be subjected to a battery of tests without a clear rationale. Sophie, for example, is only 3;2 years of age and may well be upset by the use of formal tests. Kate must therefore decide which tests might provide the most detailed evidence to help support or refute her working hypotheses. Of course the specific tests will vary according to the nature of a child’s problems. Details of different assessments are referred to in relation to specific areas of difficulty in Chapters 10–22. However, when choosing any formal assessment it is important to consider the following (Lees and Urwin 1997).
It must be age appropriate.
It should test what it purports to assess.
It must be appropriate for the child socially and culturally.
It must have been standardised on appropriate norms.
The child must have adequate attention skills to be able to concentrate for the period of time required for testing.
Is Help Needed from other Professionals to Complement/Aid Assessment?
Decision/Question: Yes/no – which Professional?
Speech and language therapists work alongside many other professionals such as audiologists, psychologists and different medical specialists all of whom may be involved in aspects of assessment. Additional input from such professionals may help the therapist to confirm or refute a hypothesis about the child’s communication problems.
For example, Kate knows it will be important for an audiologist to establish whether Sophie has any hearing difficulties and to investigate whether there have been intermittent problems at a time that was critical to her speech and language development (Moorey and Mahon 2002). If appropriate, a paediatrician or a psychologist may help to establish Sophie’s cognitive functioning levels.
When working with children with a cleft palate, a physical disability or children with severe learning disabilities, additional specialist input from members of a multi-disciplinary team may be essential for a more accurate diagnosis. (This is discussed in more detail in Chapters 10–22.)
How Should the Intervention with the Child be Managed?
Decision: The Frequency of The Intervention and where this will Take Place
Kate will share her findings with Sophie’s parents and will work in partnership with them to agree a contract regarding possible intervention. They will discuss whether further assessment and/or a therapy programme is required or whether it would be better to put Sophie ‘on review’ to be called back to check any spontaneous progress at a later date. If they decide on therapy Kate will need to agree with the parents the number of sessions, where they will take place – whether in the nursery or a health centre – and the duration of each. This will be based on Sophie’s attention span and ability to concentrate and engage in the process.
In order to make this decision Kate needs to understand the natural development of Sophie’s type of problem. For example, therapy may be expected to take a longer period if Sophie is also found to have a significant hearing loss. Kate has to ask permission from the parents before she can see Sophie in nursery. This will also give her a chance to gather further information from them. After her session with Sophie, Kate will have a follow-up discussion with the parents about how she should proceed.
Several management options would be available to Kate at this stage.
If the assessment results indicate that Sophie could make spontaneous progress, Kate may suggest a ‘wait and see’ policy. The parents could then contact her at a later date if they are still concerned, or she could agree to send a review appointment to check Sophie’s progress in several months’ time.
If Sophie appears to have ...