![]()
Part 1
Introduction
Fiona Sim and Jenny Wright
This book is an introduction to the world of public health careers. It will give you an understanding of what public health is, what issues public health practitioners are tackling and why they need tackling, a description of some of the roles and career paths that public health practitioners follow. Lastly, when you have been inspired by these roles, the book provides some signposts about where you can go to get more information.
The book is aimed at those who are starting on their career journeys and considering public health as an option, and who want more information on the range of opportunities. For those considering a move towards public health in mid-career, the book also has valuable information. It will be of interest to those who are teaching on public health courses as well as those providing careers advice to young and not-so-young people.
There is no internationally agreed definition of public health. The Alma Ata Declaration (WHO, 1978), Health for All (WHO, 1981) and the Ottawa Charter (WHO, 1986) contain the modern emphasis on securing wellbeing as well as absence of disease. Public health was defined for the UK in 1988 by the then Chief Medical Officer (CMO) in his Report of the Committee of Inquiry into the Future Development of the Public Health Function (Acheson, 1988) as ‘the science and art of preventing disease, prolonging life and promoting health through the organised efforts of society’. This was subsequently added to by Derek Wanless in his second report on public health (2004) ‘through the organised efforts and informed choices of society, organisations, public and private, communities and individuals’. With these definitions, therefore, public health has moved from being a relatively narrow discipline, based around a small professional workforce, to being the rightful consideration of the whole population.
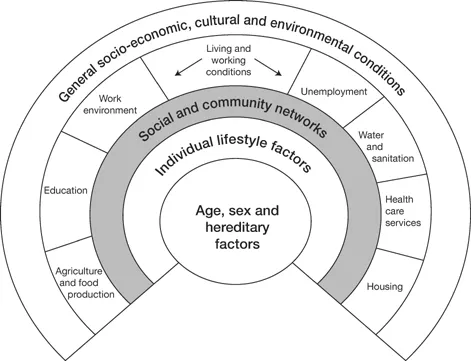
What sets public health practitioners apart is their passion and desire to improve the health and wellbeing of the population and to reduce inequalities. They want to contribute to making the world a better place. They will use their skills in understanding the impact of disease and ill health on different communities to bring about change. They are also aware of the influence of broader social and environmental factors on health, as illustrated in the diagram below (Dahlgren and Whitehead, 1991).
Figure 0.1 Dahlgren and Whitehead’s Model of the Social Determinants of Health
Source: Dahlgren and Whitehead, 1991
The book is aimed at people considering or starting their public health careers from a UK base. We recognise that the arrangements for delivery of public health goals vary tremendously around the world, so that while many of the core competencies required will be the same, the organisation of services and jobs available may be very different from one country to another. Even within the UK there are country-specific differences. The book will not dwell upon these but we highlight where they are relevant to careers.
This book will show you the rich and varied opportunities for roles and careers in public health. Public health practitioners are found working in all walks of life – in the public, private and voluntary sectors. Many make their contribution in overseas work with developing countries.
What it means to work in public health
Working in public health means working to improve everyone’s health, to prevent ill health and to make a real difference to people’s lives. This is done in many different ways, so you will see that, unlike some other occupations, there is no single job or profession that sums up ‘the public health practitioner’. What we tend to have in common, however, is a strong drive to improve the health and wellbeing of communities and an ability to have a long-term view, since many of the changes that are needed will take years or even decades to achieve.
Public health practitioners work as follows:
At local levels:
• with individuals and families;
• with and for local communities;
• with organisations that deliver services to individuals, families and communities (e.g. health services and local authorities, charities and independent organisations); and
• in teaching and research.
At regional or national levels:
• with organisations that plan services and develop policy (e.g. government departments, head offices for health services, social care organisations, charitable organisations, large companies).
At international and global levels:
• with organisations whose main focus is improving health outcomes in low- or middle-income settings (e.g. charitable organisations, United Nations organisations).
Changing public health issues
What have public health practitioners achieved for the population’s health? The public health movement really began in the middle of the nineteenth century, in the face of diseases such as cholera and at a time of very high infant mortality. The focus of nineteenth- and early twentieth-century public health had been on understanding the causes of ill health and enabling major legislation to create:
• clean water and sanitation;
• safe food;
• safe working conditions; and
• fewer infectious diseases.
During the twentieth century, as the concepts of infection and contagious diseases became better understood, initial effort focused on reducing the threat of communicable and preventable diseases by measures such as immunisation programmes covering whole populations. In the 1940s, the main determinants of poor health were described in the Beveridge Report (Beveridge, 1942) as the ‘Five Giants: Squalor, Ignorance, Want, Idleness, Disease’.
One major public health achievement in the UK at the end of the century was the introduction of seat-belt legislation to promote safety on roads. In the twenty-first century, the ban on smoking in public places has been an important step forward, in response to increasing understanding and political acceptance of the harmful effects on people’s health from ‘second-hand’ tobacco smoke.
As a result of public health interventions, people are living longer and are healthier for longer, and there are fewer infant and child deaths, but there remain large inequalities in health between different groups within and between populations.
In the twenty-first century we have, however, a new set of challenges for the public health workforce in developed countries:
• management of chronic diseases and the impact of an ageing population;
• risks from new and emerging infectious diseases such as the severe acute respiratory syndrome (SARS) outbreak in 2002 and pandemics such as swine flu;
• climate change and its impact on health;
• widening inequalities in health, with poorer people being likely to have worse health and to live shorter lives than those who are more affluent;
• rapidly evolving lifestyle threats such as obesity and binge drinking of alcohol, as well as the continuing challenges posed by tobacco.
Global burden of disease
The average global life expectancy at birth is now 70 years, ranging from 60 years in low-income countries to 80 years in high-income countries (WHO, 2014). In many countries, more commonly low-income countries, there is no routine registration of diseases or of deaths and their cause, so that, while estimates are made, it is impossible to know accurately what diseases cause most ill health among populations worldwide, or which cause most deaths.
In the UK, and in many other high-income countries, information has been collected for decades that allows the health of the population to be tracked. Over time, the number of deaths from infectious diseases has declined – much of the improvement as a result of public health interventions such as clean water, better food hygiene and population-wide immunisation programmes – but deaths due to modern epidemics of heart disease, stroke and cancer have increased. Most of these modern scourges are linked with changes in society that have led to changes in diet, increased access to alcohol and tobacco, and lack of physical activity. Death is only one measure of health, of course, and the number of people who suffer long periods of ill health, particularly in older age, due to long-term conditions such as diabetes, circulatory diseases and dementia, are now of great importance to individuals and their families, and to the national economy, due to their major impact on demand for health and social care services. Unfortunately, the dream of the founding fathers of the NHS, who thought that the population would steadily become healthier and the need for healthcare would diminish, was somewhat flawed as many people live longer, but in poorer health. For public health practitioners the greatest challenge is to achieve healthy longevity – ‘adding life to years as well as years to life’ (Sim and McKee, 2011).
In response to these challenges, we need competent public health practitioners, working at all levels and in all settings. Whatever field of public health they work in, practitioners will need the following:
• awareness of differing health needs;
• knowledge of what influences our health and wellbeing;
• understanding of how to prevent ill health and promote health.
They will need skills in:
• communicating effectively;
• working successfully in collaboration with others, to influence and negotiate;
• analysing and interpreting information on people and health;
• reviewing literature on what makes a difference.
Introducing the public health workforce
The workforce is multidisciplinary, which means that public health practitioners come from a very wide range of initial disciplines and backgrounds. This can include medicine, nursing and other health professions, teaching, management, pharmacy, science, geography, mathematics, nutrition and the civil service. Increasingly, recruits to the pu...