Mental Health and Physical Health are undeniably connected. One cannot recover physically, if there is still mental suffering, and vice versa. The essays collected here examine the relationship between mental and physical health, and how that relationship flourishes or suffers in a managed care environment. Understanding more about how the psychological aftereffects of an illness, and the best ways to respond to them, will ultimately enhance the care offered to patients. The contributors offer a wide range of examples of linked physical and mental illnesses, with advice on how best to responsibly address and treat both.
Clinicians and practitioners will welcome this guide to navigating a managed care system and working with patients to heal both their mental and physical maladies equally.

eBook - ePub
Psychosocial Treatment for Medical Conditions
Principles and Techniques
- 352 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Psychosocial Treatment for Medical Conditions
Principles and Techniques
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Print ISBN
9781583913666
Subtopic
Mental Health in PsychologySECTION II
Medical Conditions
CHAPTER 3
Psychosocial Sequelae of Cancer Diagnosis and Treatment
Each year in the United States, over one million new cases of cancer are diagnosed and more than 500,000 people die of cancer (American Cancer Society, 2002). Malignant disease is the second most common cause of death in America; only heart disease takes more lives. However, the picture is not completely grim. The number and percentage of cancer survivors in the U.S. increases annually, and is estimated to be about 8 million (American Cancer Society, 2002). Many of these individuals can be considered cured of their disease. In other words, cancer is no longer present and their disease is not expected to recur. Even if not cured, the length of time between diagnosis and death has been extended for many people with cancer. The combination of high incidence, high mortality, and large numbers of individuals living with cancer for an extended period of time has increased the attention that must be paid to the psychological and social ramifications of malignant disease.
This chapter will review and examine the psychosocial impact and sequelae associated with the diagnosis and treatment of cancer. To begin, however, we will provide a brief overview of cancer as well as current cancer treatment.
CANCER: BASIC MEDICAL CONSIDERATIONS
While cancer may strike individuals at any time in life, it is primarily a disease of aging. The typical age at which cancer is initially diagnosed is in the 50s and 60s for the most common cancers. The natural history of one type of cancer may vary widely from another type, but all malignancies share abnormalities in growth characteristics. Malignant cells must be evaluated with regard to two separate but often linked properties: (1) the speed and ability to grow locally in an unregulated manner; and (2) the ability to invade adjacent tissues and other organs. The mortality rate of some cancers results primarily from uncontrolled growth at the site of cancer development (e.g., pancreatic cancer). Others (e.g., colon cancer and breast cancer) may be localized at initial diagnosis but have the potential to metastasize to other sites in the body and become fatal with time. Still other cancers are systemic and often widespread at the time of diagnosis (e.g., leukemias and lymphomas).
When cancer is suspected, a sample of the abnormal tissue is obtained using one of several biopsy techniques (see Table 3.1). In general, the least invasive method is used. This general principle results in the use of different diagnostic tests in different malignancies. Different diagnostic tests are also used in patients with the same malignancy who show varying signs and symptoms.
TABLE 3.1. Techniques Used to Diagnose Malignancy
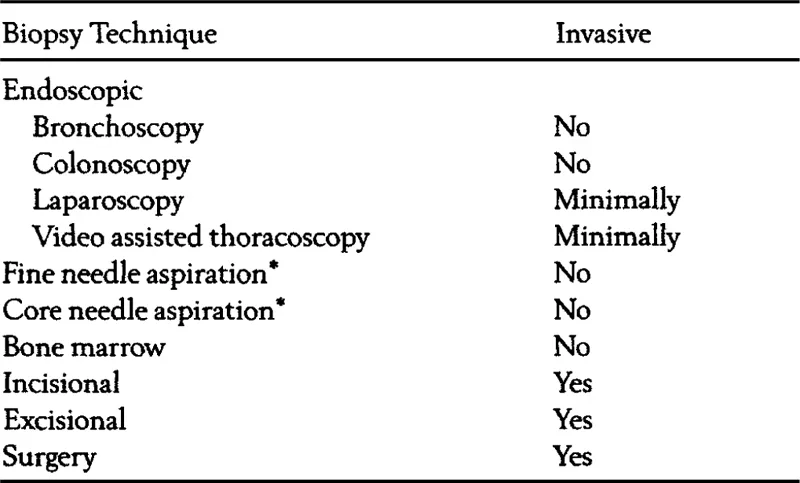
* May be performed on palpable lesions or nonpalpable lesions with X-ray (CT scan, mammogram) guidance.
The tissue obtained in the biopsy is then carefully evaluated by a trained pathologist to ensure that the correct diagnosis is made and that the disease is correctly staged. Staging involves classification of a malignancy with regard to its size and extent of local, regional, and distal (or metastatic) spread. Local disease refers to tumors that are usually small and have not spread beyond the original organ involved. Regional disease refers to tumors that have spread beyond the initial organ site into adjoining tissue or nearby lymph nodes. Distal (or metastatic) disease refers to tumors that have spread beyond the initial organ site into not only adjoining tissue or regional lymph nodes, but to other more distant body or organ sites as well. Staging information is critical to determine which therapy will be most effective, as well as the patient’s likely prognosis.
A variety of modalities are used in treating cancer, each with their own acute and chronic side effects (see Table 3.2). In general, cancer treatment involves a combination of surgery, chemotherapy, and radiotherapy. Additionally, hormonal therapy may be used for cancers of the breast or prostate. In selecting a therapy, the age and general health of the patient are considered. In considering the patient’s general health, the patient’s Karnofsky Performance Status score is important. The Karnofsky Performance Status score rates a patient’s ability to perform routine daily activities, such as walking, lifting, or feeding and clothing himself or herself. The Karnofsky score can predict how well cancer therapy will be tolerated as well as its efficacy (Schag, Heinrich, & Ganz, 1984).
TABLE 3.2. Cancer Treatment Modalities

* May be any combination of above therapies.
A diagnosis of cancer can be emotionally devastating. Psychological and emotional sequelae must be anticipated by the multidisciplinary health care team and managed appropriately. The team must be prepared to treat the cancer patient for pain, dehydration, depression, and other psychological and social sequelae. The team must also educate the patient, the family, and other caregivers about these problems. The health care team must share with the patient and his or her family the goals of therapy. Patients diagnosed with incurable malignancy may obtain relief from symptoms and have prolonged survival with therapy. However, the side effects of therapy must be weighed against the benefits. Patients with a curable malignancy may be willing to tolerate greater short-term side effects to achieve the benefits of a longer life.
Cancer is a very broad term that covers over 100 different diseases. Despite this diversity, all cancers involve a defect in the normal biological mechanisms that control the growth and differentiation of normal human cells. This section will provide a brief medical overview of some of the more common malignancies, with information provided regarding the nature and course of the disease, major diagnostic procedures, staging, and major forms of treatment. Readers desiring more information are referred to a comprehensive handbook edited by DeVita and colleagues (DeVita, Hellman, & Rosenberg, 1997). Tables 3.3 and 3.4 present basic epidemiological information regarding some of the more common cancers we will review. Table 3.3 presents information regarding incidence and mortality. Table 3.4 presents information regarding the proportion of patients surviving five or more years following a cancer diagnosis.
TABLE 3.3. Estimated Incidence and Mortality Associated With Specific Cancer Diagnoses in 2002 (in Thousands)
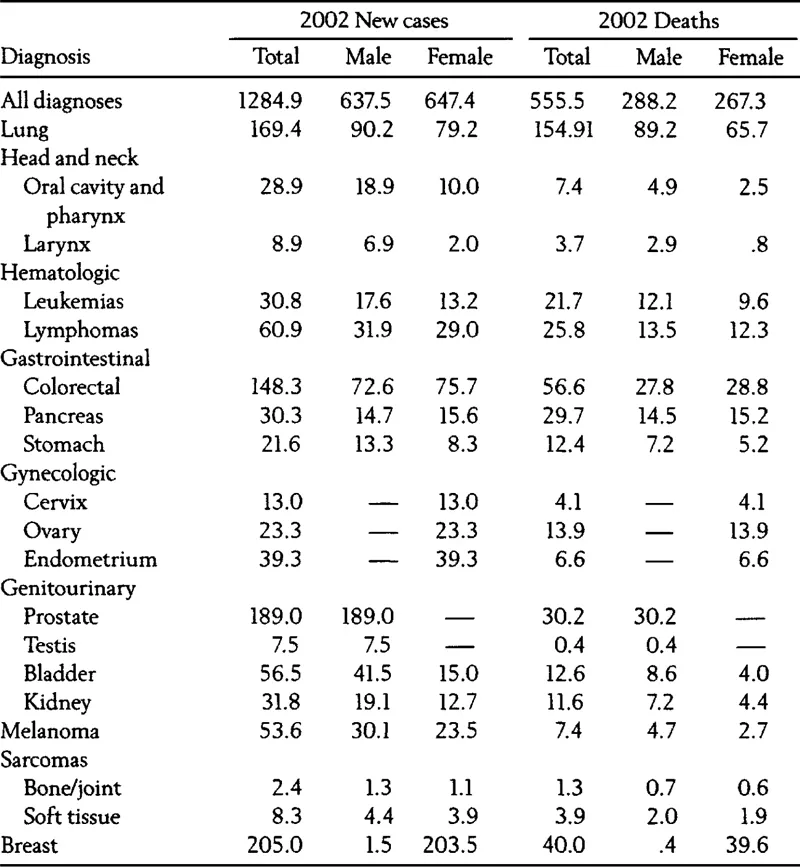
Note: Data is estimated new cases and deaths in 2002 from American Cancer Society (2002).
Source: From the American Cancer Society’s Cancer Facts and Figures, 2002. Reprinted with permission.
TABLE 3.4. Percentage of Individuals Surviving at Least Five Years Following Diagnosis of Various Cancers By Stage at Diagnosis (American Cancer Society, 2002).
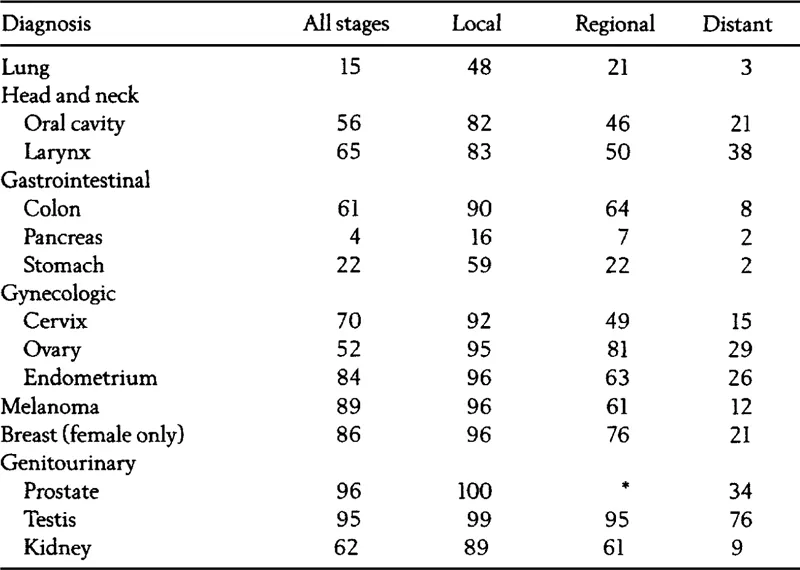
Note: Percentages are adjusted for normal life expectancy.
* The rate for local stages of prostrate cancer represents local and regional stages combined.
* The rate for local stages of prostrate cancer represents local and regional stages combined.
Source: From the American Cancer Society’s Cancer Facts and Figures, 2002. Reprinted with Permission.
Lung Cancer
Lung cancer is the third most common type of cancer but it is the most common cause of cancer death in the United States. Lung cancer constitutes approximately 13% of all cancers diagnosed in the United States. In 2002, there were 169,400 new cases of lung cancer diagnosed in the United States, with 154, 900 individuals dying of the disease (American Cancer Society, 2002). Carcinoma of the lung originates in epithelial cells lining the bronchia. There are no proven methods to screen for the disease. Lung cancer patients typically present with cough, often with traces of blood in the sputum, shortness of breath, chest pain or weight loss, but the cancer is usually advanced by that time. Occasionally, when the disease is in an advanced stage, a chest X-ray obtained for an unrelated reason will show a mass, leading to the subsequent diagnosis of lung cancer.
Tissue may be obtained for diagnosis in a number of ways—bronchoscopy, needle biopsy, or surgery. Microscopic exam of the tissue allows the pathologist to determine if the histologic type is squamous cell, adenocarcinoma, large-cell, or small-cell type. Patients diagnosed with small cell-lung carcinoma must be treated systemically (i.e., with chemotherapy) as this type of lung cancer spreads through the blood stream. Therapeutic decisions for patients with other types of lung cancer will be made based on the stage of disease when found. Patients with local disease, confined to the bronchia or directly adjacent lymph nodes, are evaluated for local therapies (i.e., surgery and radiation). Patients must also be evaluated for metastasis to nonadjacent lymph nodes, bone, liver, and brain. Patients with disease at these sites may be offered systemic therapy (i.e., chemotherapy) combined with local treatments such as surgery and/or radiation.
Recent statistics suggest that only 15% of all individuals diagnosed with lung cancer survive at least five years following diagnosis (American Cancer Society, 2002). The likelihood of surviving five years after a diagnosis of lung cancer is effected by disease stage, the presence of other medical conditions such as chronic obstructive airway disease, and the effectiveness of therapy. Patients di agnosed with early (stage I) disease are often cured of their disease with surgery. Patients diagnosed with advanced (stage IV) disease have a median survival of 8 to 12 months even when treated systemically with chemotherapy.
Head and Neck Cancers
Cancers of the head and neck constitute approximately 3.4% of all cancers diagnosed in the United States. In 2002, 37,800 new cases of head and neck cancer were diagnosed in the United States with 11,100 individuals dying of this cancer (American Cancer Society, 2002). Head and neck cancers include those of the oral cavity, pharynx, sinuses, larynx, salivary glands, or skin of the face and neck. Presenting symptoms vary with site of disease and range from a skin lesion to hoarseness. Staging involves evaluation by a physician specialized in examination of the aerodigestive tract (e.g., otolaryngologist or ENT specialist). Patients with head and neck cancer may have multiple primary tumors (Vokes, Weichselbaum, Lippman, & Hong, 1993). Hence, surgery and radiotherapy are the optimal treatments. Surgical cure may require sacrifice of tissues crucial to speech and nutrition. Accordingly, a multidisciplinary team including a plastic surgeon, speech therapist, nutritionist, and oral surgeon maybe required to construct a prosthesis and to support physical and emotional recovery. Control of local or regional disease is especially challenging in head and neck cancers as the risk of relapse is high. In general, risk of local relapse after aggressive therapy is related to the size of the primary tumor and the extent of lymph node involvement. Chemotherapy is generally reserved for patients when surgery and radiotherapy has failed to control their disease.
Recent statistics indicate that the percentage of patients who live for five years following diagnosis of cancer of the larynx or oral cavity is 65% and 56%, respectively (American Cancer Society, 2002). Again, however, five-year survival is highly dependent upon the stage of disease at diagnosis. Five-year survival for both types of cancers for patients with local disease at diagnosis exceeds 80%. In contrast, five-year survival for patients with distal (i.e., metastatic) disease at diagnosis is 38% for cancer of the larynx and only 21% for cancers of the oral cavity.
Hematologic Cancers
Hematologic malignancies include acute and chronic leukemias as well as both Hodgkin’s and non-Hodgkin’s lymphomas. Patients with these diseases are typically categorized together as these diseases involve the bone marrow and lymphatic system. Hematologic malignancies comprise 7.4% of all cancers diagnosed in the United States. In 2002, 91,700 new cases of leukemia and lymphoma will be diagnosed in the United States with 47,500 individuals dying of these cancers (American Cancer Society, 2002). Hematologic malignancies are often curable even in advanced stages.
Patients with hematologic cancers typically present with symptoms of fever, night sweats, weight loss, reduced appetite, and abnormalities in the complete blood count. Leukemia originates in the bone marrow and therefore is always a systemic disease. The diagnosis of leukemia may be made by demonstration of premature or very young cells (blasts) in the peripheral blood or bone marrow. Leukemia is associated with abnormalities in white blood cells, red blood cells, and platelets, resulting in increased risk of infection, anemia, and bleeding. Patients with acute leukemia present with dramatic evidence of these abnormalities such as nosebleeds, bleeding from the mouth or gums, or life-threatening infection. These patients have only a short history of illness. Individuals with acute leukemia require immediate support with blood products, antibiotics, and chemotherapy. Patients with chronic leukemia may present with less dramatic symptoms and often have a history of a long period of fatigue. Those with chronic disease may be observed without treatment for some time before therapy is required. The untreated natural history of acute leukemia is a short, severe, life-threatening illness; however, the disease is cured in approximately 50% of patients. The natural history of chronic leukemia is more lengthy and less symptomatic. Patients may live for many years after their diagnosis. Their disease is often responsive to chemotherapy initially but becomes more resis tant over time. Most patients with chronic leukemia will eventually die of their disease. Young patients in good general health with either acute or chronic leukemia may be candidates for high-dose chemotherapy followed by bone marrow transplantation.
Lymphoma may be of the...
Table of contents
- Cover
- Halftitle
- Title
- Copyright
- Dedication
- Contents
- Contributors
- Foreword: Mind Matters
- Preface
- Section I. Introduction
- Section II. Medical Conditions
- Section III. Treatment
- Section IV. Summary
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Psychosocial Treatment for Medical Conditions by Leon A. Schein, Harold S. Bernard, Henry I. Spitz, Philip R. Muskin, Leon A. Schein,Harold S. Bernard,Henry I. Spitz,Philip R. Muskin in PDF and/or ePUB format. We have over 1.5 million books available in our catalogue for you to explore.