![]()
Chapter 1
Activities and Adaptation: A Call for Innovations to Serve Aging Adults with Developmental Disabilities
Barbara A. Hawkins
Phyllis B. Kultgen
Barbara A. Hawkins, ReD, is Assistant Professor of Recreation at Indiana University, and Director of the Program on Aging and Developmental Disabilities, I.U. Institute for the Study of Developmental Disabilities. Dr. Hawkins serves as Associate Editor for the AALR/ATR Annual in Therapeutic Recreation and the Therapeutic Recreation Journal, and is Author/Editor of Aging and Developmental Disabilities — A Training Inservice Package. Phyllis B. Kultgen, PhD, is Director of Training for the Program on Aging and Developmental Disabilities at the Institute for the Study of Developmental Disabilities — Indiana University. Dr. Kultgen has authored several training manuals in the area of aging and DD, and is a contributing author to Aging and Developmental Disabilities — A Training lnservice Package.
SUMMARY. Aging in people with developmental disabilities has emerged as a new area of concern within the past two decades. Little is known, however, about the influence of aging for this population, especially in terms of planning and delivering appropriate activities. This article briefly overviews characteristics of the population. It further describes exemplary program strategies from three areas: companionship, physical activity, and retirement preparation. Challenges to activity professionals are suggested.
INTRODUCTION
During the past two decades, service providers in the developmental disabilities (DD) system have become increasingly aware of the aging phenomenon as it has begun to significantly impact this population group. At a recent national symposium, Ray (1990)pinpointed this area as one of ten top trends and issues for leisure service providers in the decade to come. The increased attention, within the past few years, by recreation professionals to this group holds promise for the development of needed activity programs that can be adapted for the dual phenomenon of aging and developmental disabilities (Benz, Halpern, & Close, 1986; Boyd & James, 1990; Hawkins, 1987 & 1989a; Rancourt, 1989 & 1990).
Not only is a greying of the population a trend for the larger society but also a new direction for people who have been develop-mentally challenged throughout their lives. This changing course in demography is particularly poignant in light of the historical context for people who have mental retardation or some other developmental disability. Formerly, for these people, life expectancy was typically short and tenuous. In more recent decades, as treatment models have emphasized habilitation and humane treatment, people with developmental disabilities are surviving into adulthood and many are reaching later maturity. With the emergence of significant numbers of aging and aged adults with developmental disabilities has come the need for new information, collaborative efforts between the aging and DD networks, and trained professionals from both service sectors to deliver appropriate programs.
This chapter provides an overview of the background information on the older DD population. Program strategies that have been developed and are being evaluated will be presented. Research and program innovations that are needed will be suggested with some implications drawn for activity professionals.
POPULATION BACKGROUND
It has been estimated that the size of the older adult population with developmental disabilities for the nation in 1980 was around 200,000 (Janicki, Seltzer, Krauss & Gaetani, 1989). Problems with the estimation of size have been widely discussed in the literature and include the lack of reliable national studies on which to establish age adjusted prevalence rates as a concern (Jacobson, Sutton, & Janicki, 1985; Janicki, Krauss, & Seltzer, 1987; Lubin & Kiely, 1985; Rose & Janicki, 1986). Existing prevalence rates have varied from 34% to 3% (DiGiovanni, 1978;Rose & Janicki, 1986) for the population. Based on the 1980 census, these rates yield a very broad range in potential size from 200,000 to 1.4 million people. An accurate, as opposed to estimated, prevalence rate that is adjusted distinctly for age is needed; particularly, as it will provide a more accurate assessment of the population size.
In spite of the problems associated with determining the actual size of this group, numerous state-level assessment and planning efforts have been made in recent years (Hawkins & Eklund, 1989, 1990). These studies have done much to describe the needs and attributes of the population. They serve as a benchmark in the planning and public policy development process that usually accompanies population groups that have the need for government-sponsored human services. These services include health care, living arrangements, rehabilitative and habilitative care, advocacy and protection, and other support services such as case coordination and transportation.
In spite of the problems associated with determining the actual size of this group, numerous state-level assessment and planning efforts have been made in recent years (Hawkins & Eklund, 1989, 1990). These studies have done much to describe the needs and attributes of the population. They serve as a benchmark in the planning and public policy development process that usually accompanies population groups that have the need for government-sponsored human services. These services include health care, living arrangements, rehabilitative and habilitative care, advocacy and protection, and other support services such as case coordination and transportation.
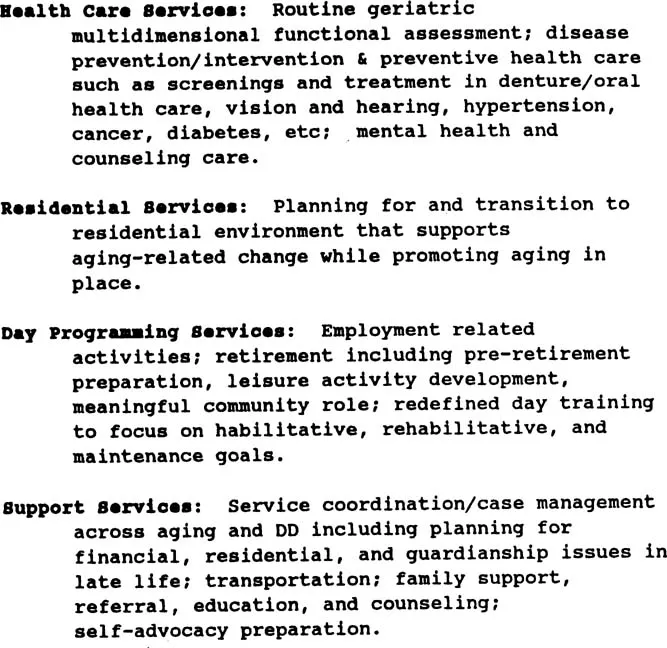
The identified service areas (Hawkins & Eklund, 1990) that aging and older people with developmental disabilities typically need include those that are listed in Figure 1. These services relate to both the aging process and the presence of developmental disability, and may be exacerbated by these circumstances in combination.
To better understand service needs, it will be helpful to review characteristics of aging and older adults with developmental disabilities. Most of the research on aging processes in people with DD, however, has been done on people who have mental retardation as their primary diagnosis (Janicki, Seltzer, Krauss & Gaetani, 1989). There remains a dearth of research information about aging processes in persons who have other lifelong disabling conditions such as cerebral palsy, epilepsy, and autism. Thus, it is important to keep in mind that much of what follows pertains to people with mental retardation.
Health, Physical, and Behavioral Characteristics
The research evidence on physical functioning and health status for people with mental retardation who are aging presents a mixed
FIGURE 1. Service Needs of Aging/Aged Adults with DD
picture. Some studies suggest little difference between aging people with and without mental retardation on health status (Anderson, Lakin, Bruininks, and Hill, 1987). Krauss and Seltzer (1986) found that older adults had fewer medical problems than younger adults with mental retardation with the exception of sensory impairments. However, Janicki and MacEachron (1984) found that the older adults used medical services more than did younger adults. These conflicting findings may be confounded by the place of residence (institutional, group home, natural family), accessible medical services, geographic location (rural, urban), or selected attributes of the cohort studied.
In spite of conflicting results among both cross sectional and longitudinal studies on functional status, contemporary viewpoints support observable declines in motoric and sensory function apparent in people in their fifties. Other behavioral skills, however, are maintained and may even continue to improve (i.e., daily living skills and intellectual functions) until the seventh decade. The severity of mental retardation or developmental disability, as well as cohort effects (i.e., long periods of institutionalization), may influence the degree of decline and thus, overall life expectancy (Janicki & Jacobson, 1986; Krauss & Seltzer, 1986; Eyman & Widaman, 1987).
While design weaknesses are evident in the current available research (Seltzer, 1985), developmentally challenged people who live into older adulthood do not appear to be drastically different in their physical, health, and behavioral needs from other elderly people. The implication from this finding is that many existing programs and service strategies hold promise for meeting the needs for this population group in terms of daily health, physical, and behavioral functions.
Social Function and Support Characteristics
For the general population of elderly people, social support and social activities revolve around informal caregivers (i.e., family members, neighbors, friends) and the senior services network. For aging and older people with developmental disabilities, this pattern is markedly different.
Most elderly people with developmental disabilities no longer live at home, nor do they have spouses and adult children who can provide social support for them. While Seltzer (1989a, 1989b) and Krauss (1989) have reported preliminary evidence on the differences between the support networks of aging adults with mental retardation compared to the general population, these findings are some of the first to be produced in the research arena.
Little is known about the patterns and changes in sibling involvement over the lifecourse of aging adults with DD. The social relationships that do exist for this population tend to consist of co-residents in congregate residential facilities, friends at work or day activity centers, and paid caregivers (Rinck & Kultgen, 1987). The lack of a stable social support network is one of the most troubling concerns of older adults with DD.
Also, little is known about the retirement and leisure activity involvement of members of this population group. The role of recreational and leisure activities as core components of a habilitation plan, particularly as vocational objectives lessen in prominence, is an area for research. Ascertaining needs, interests and functional skills that promote free time use, as well as maintain other functional and behavioral skills, may well be one of the most critical areas for program development. Some research evidence (Hawkins, 1989) suggests that older adults with mental retardation have a wide range of leisure interests but may be constrained by the lack of friends or equipment needed to pursue those interests. Additional constraints include the lack of instruction in how to perform preferred activities and lack of choice in selecting activities.
Clearly, in terms of social function and activity involvement, the lives of elderly people with DD are not parallel to the general elderly population (Foelker & Luke, 1989). Older adults with DD, however, do experience feelings of grief and adjustment to changes in their own functioning as well as to other losses (i.e., death of friends, family) that are common in later life stages (Menolascino & Potter, 1989). Residential relocation (i.e., transition trauma), removal of work related social networks, the lack of a family support network, and the variable presence of a well developed pattern of leisure activity involvement may heighten awareness of vulnerabilities associated with being developmentally challenged and living a long life.
EXEMPLARY PROGRAM STRATEGIES
Based on known vulnerabilities for people who are old with DD, three broad areas in which exemplary programs have been developed will be discussed. These three areas encompass companionship/friendship, physical functioning, and retirement adjustment. Programming strategies in these three areas are innovative because they address the specific concerns of older adults who have lived with lifelong disabling conditions that have constrained the development of normalized lifestyles and patterns. Thus, innovations in these programs are reflective of important needs for aging adults with DD and represent creative solutions to a changed focus in habilitation planning. Each of these areas are special areas in terms of their contribution to adjustment, overall health, functioning, and quality of life in older adulthood for people who have DD.
Companionship/Friendship
In response to the constricted informal social support networks of older persons with developmental disabilities, a number of demonstration companionship/friendship projects emerged during the decade of the 1980s. The aim of such programs has been to expand opportunities for both community participation and peer companionship. The emergent model projects are considered innovative because of the emphasis given to friendship pairing between an elder from the local community and an older person with a disability.
The Community Access Program, originating in Akron, Ohio under a grant from the Joseph P. Kennedy, Jr. Foundation (Stroud and Sutton, 1988), uses peer companions, either volunteer or employed, to accompany older persons with mental retardation into the community. These “senior friends” introduce people with disabilities to the wide range of leisure and recreational activity options that exist beyond the boundaries of their sheltered residential setting. Community activities in this model may include participation in specifically designated senior activities (i.e., senior centers, golden age clubs, senior exercise) or in community-wide leisure and recreational options.
The Companion Program developed across mid-Missouri through funding from the Administration on Aging (Ku...