Compassionate communities are communities that provide assistance for those in need of end of life care, separate from any official heath service provision that may already be available within the community. This idea was developed in 2005 in Allan Kellehear's seminal volume- Compassionate Cities: Public Health and End of Life Care. In the ensuing ten years the theoretical aspects of the idea have been continually explored, primarily rehearsing academic concerns rather than practical ones.
Compassionate Communities: Case Studies from Britain and Europe provides the first major volume describing and examining compassionate community experiments in end of life care from a highly practical perspective. Focusing on community development initiatives and practice challenges, the book offers practitioners and policy makers from the health and social care sectors practical discussions on the strengths and limitations of such initiatives. Furthermore, not limited to providing practice choices the book also offers an important and timely impetus for other practitioners and policy makers to begin thinking about developing their own possible compassionate communities.
An essential read for academic, practitioner, and policy audiences in the fields of public health, community development, health social sciences, aged care, bereavement care, and hospice & palliative care, Compassionate Communities is one of only a handful of available books on end of life care that takes a strong health promotion and community development approach.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Libby Sallnow, Antonia Bunnin and Heather Richardson
DOI: 10.4324/9781315735801-1
Community and hospices
In the UK, the notions of hospice and community are closely intertwined at conceptual, strategic and operational levels. Many hospices in this country owe their origins, early funding and initial plans to local people or groups who had a vision to create a new service for people dying in their area and who were prepared to donate time, money and effort to make this vision a reality. Such community support remains vital for the majority of hospices even as they are well established and employ large numbers of professionals to deliver care and manage the business of the organisation. Today, nationally, 74 per cent of funding for independent hospices operating in the UK is raised from charitable rather than statutory sources (Hospice UK, 2014), including a significant proportion from community fundraising. Opportunities for, and numbers of, volunteers working in hospices also continue to grow. It is estimated that the UK hospice volunteer workforce now exceeds 125,000 people (Help the Hospices, 2014), who take on a variety of roles including fundraising, care delivery, retail support, contributions as unpaid professionals and governance (Hoad, 1991; Turner and Payne, 2008; Burbeck et al. 2014). The annual financial value of their contribution has been estimated at £133 million in return for an investment of £16.7 million (Gaskin, 2003). The contribution of volunteers is recognised as extending beyond pure financial gains, however, and the impacts on patients and families (Herbst-Damm and Kulik 2005; Block et al., 2010; Candy et al., 2014), on the volunteers themselves (Addington-Hall and Karlsen, 2005; Harris and Thoresen, 2006; Li, 2007) and on broader issues such as social ties and support (McKinnon, 2002) have been widely documented.
This vital relationship between hospices and communities is recognised by the hospice sector. The national umbrella organisation for hospice care – Hospice UK (formerly Help the Hospices) has placed an emphasis on the relationship that hospices have with the communities they serve by highlighting it in its definition of hospice care as ‘community engaged palliative and end of life care in all settings for patients, families and carers’ (Help the Hospices, 2012a). This was intended as a means of differentiating hospice care from other forms of palliative and end of life care. Most hospices have put a variety of structures and processes in place to connect the organisation to local people and community groups – including volunteer coordinators and community fundraisers.
Volunteering and hospices
Volunteering, seen as one of the main conduits of connection between hospices and their local communities, has recently come under closer scrutiny with the recognition that the wider impacts of volunteering, besides the financial gains, may be worth investigation (Leadbeater and Garber, 2010). Traditional models of volunteering within hospices focus on recruiting volunteers to fulfil roles required by the hospice, to support them in their service delivery. Differing models from around the world (see Kumar, 2007; and Jack et al., 2011) have prompted many to re-evaluate their current models of volunteer ‘management’ and to ask whether this resource could be managed differently, to provide benefits beyond the hospice, to the wider community. In so doing, hospices move towards a community development approach.
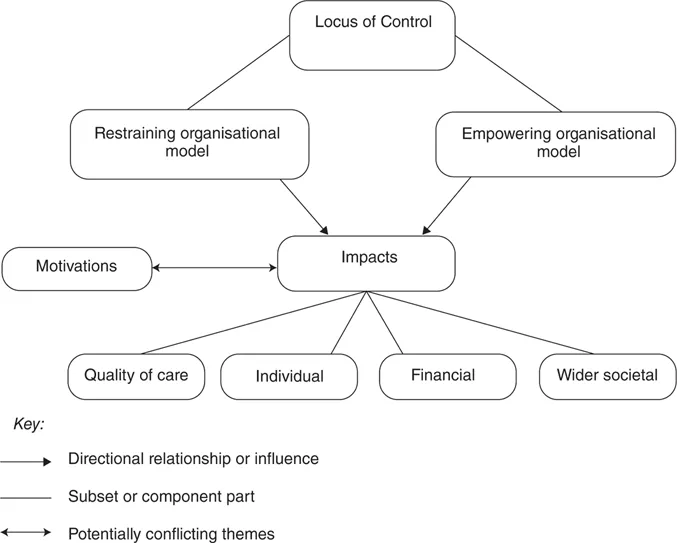
Sallnow (2010) conducted a systematic review of the literature relating to volunteering in palliative care internationally and developed a conceptual model regarding how volunteering could be understood (Figure 1.1). The literature demonstrated that there are a range of impacts beyond the financial, including wider societal implications. It also demonstrated that key factors in determining what impacts are realised are the motivations and experiences of the local people volunteering and type of management style that governs it. A style that focuses on power sharing and respecting the volunteer as presenting a unique contribution from the local community (an empowering model of management) would be more able to realise these loftier aims of social change, whereas a more restraining model, where the hospice sets the agenda and volunteers arrive to fit predetermined slots, will be less able.
The Commission into the Future of Hospice Care confirmed a need to develop new approaches to volunteering, including models of hospice-owned but volunteer-led services (Help the Hospices, 2012b).
This reappraisal of the role of volunteers within hospice care can be seen to be part of a wider, national refocusing on the relationship people as citizens, rather than patients, have with their statutory, voluntary and other organisations. Involving local people in the decisions that affect them has been included in government papers (Cabinet Office, 2009, 2010; Department of Health, 2011), grass-roots community projects (Social Action for Health, 2012) and research (Oliver et al., 2007) and the impact this can have in health and social care has not gone unnoticed. The links between social support or social networks and health have been demonstrated (Holt-Lunstad et al. 2010; Reeves et al., 2014) and, increasingly, evidence is suggesting that engaging communities in tackling health issues leads to better results than leaving it solely to professionals (O’Mara-Eves et al., 2013). The findings of reviews such as the Marmot Review (2010) confirm that in order to tackle health inequalities most effectively, local participatory decision making must be enabled. This recognition has led to multi-level policy initiatives in the UK, from the creation of Health and Wellbeing boards being tasked with tackling social isolation (Department of Health, 2012; Buck and Gregory, 2013) to social prescribing (South et al., 2008) to the NHS Alliance releasing its first Community Development Charter (NHS Alliance, 2014), calling on organisations from NHS England to individual commissioners to prioritise the engagement of local people.
Figure1.1 A conceptual model of volunteering
Source: Copyright Libby Sallnow, 2010.
Community development and hospices
The role and importance of engaging communities in their own end of life care has been expounded within palliative care since the 1990s and the sector is now looking beyond models of volunteering to radically different means of engagement. Kellehear (1999, 2005; Karapliaglou and Kellehear, 2014) first explicitly aligned the two seemingly contradictory disciplines of public health and end of life care. Services have then taken this ‘new’ public health approach, namely one that focuses on a health promoting approach as outlined in the Ottawa Charter (WHO, 1986), and applied the same principles of building healthy public policy, creating supportive environments, strengthening community action, developing personal skills and reorienting health services to contemporary end of life care. Examples of such applications exist around the world (Sallnow et al., 2012; Horsfall et al., 2012; McLoughlin, 2013).
Later chapters in this book confirm an increasing interest in new public health in the UK. The predominant interpretation of the public health approach across its four nations has been through ‘strengthening community action’, or community development, and this has come to be known under the collective heading of ‘compassionate communities’. A recent surge in interest and commitment to this approach is evident across the sector (Paul and Sallnow, 2013; Barry and Patel, 2013).
Compassionate communities and their potential contribution to the hospice sector
Although the hospice sector has made unparalleled advances in the care and support of the dying and their families since the start of the modern hospice movement in the late 1960s, questions remain about the extent to which hospices are delivering on their original goal and purpose, and to what extent those original goals are relevant for the different context and environment we find ourselves in today.
The challenges of the twenty-first century are placing new and heavier demands on already stretched health and social care services. A report written by Calanzani et al. (2013) describes a future in which there will be increasing numbers of people who live for extended periods with chronic and life-threatening conditions, many living alone with high levels of disability. The epidemiological transition means we are seeing chronic conditions such as heart disease, cancer and dementia with long trajectories rather than acute forms of infective illnesses with relatively shorter durations. The burden this places on health and social care services is significant, as they were predicated on an acute model of illness. Another corollary of our ageing population is the emergence of social isolation as a major public health concern (Cattan et al., 2005). The rise of single-person households and housebound individuals at the end of life means this is an urgent concern for the field.
The hospice sector has faced criticism over its poor record of access by people from minority ethnic groups (Coupland et al., 2011), those from lesbian, gay, bisexual and transgender (LGBT) communities (Harding et al., 2012), from those with conditions other than cancer or of older people (Ahmed et al., 2004), and low social economic class (Kessler et al., 2005). Indeed, hospice care has been labelled ‘deluxe dying for the few’ (Douglas, 1992). Sustained efforts to tackle these issues have led to important changes, for example work by St Joseph’s Hospice in East London to increase access for people from minority ethnic groups in the area (Richardson, 2012), but the sector acknowledges that there remains more to be done (Help the Hospices, 2013).
Hospices have also been subject to the critique that they have contributed, albeit unwittingly, to the disempowerment of communities and individuals in relation to end of life care. By professionalising the business of dying, families and communities are pushed to the peripheries as the professionals are viewed as the only ones who can support someone who is dying. Coupled with this is the concern regarding the medicalisation of palliative care, with critics suggesting that medical or psychological symptom management is prioritised at the expense of social issues. Kellehear (1999) writes convincingly of the gap that is emerging in a model of care that fails to acknowledge the social experience of dying and loss and which is concerned almost entirely with the management of physical symptoms. This tension extends beyond care of the dying person to those who face loss. Nyatanga (2014) warns the palliative care world of pathologising grief and seeking to manage it, rather than seeing it as a natural process with inevitable chaos. This, combined with the fear local communities may have about their role and what they are allowed to do when someone is dying, means communities step back and ask for professional support, even though they may have been fulfilling a particular role for a person for many years. Recently, there has been increasing realisation that these community roles and strengths need to be supported and that professionals should endeavour to fit into the gaps around them. This requires a different approach, to look at strengths and assets, rather than just needs. The NHS Alliance suggests ‘looking at what is strong and not wrong’ (NHS Alliance, 2014).
Finally, the current fiscal climate means hospices and other voluntary organisations are struggling to provide a comprehensive service with current funding streams. With the predicted increases in deaths year on year, the current models of inpatient, specialist palliative care will not be able to meet these demands ...
Table of contents
Cover Page
Halftitle Page
Series Page
Title Page
Copyright Page
Table Of Contents
List of figures
List of contributors
Preface
1 Community development and hospices: a national UK perspective
2 Developing community support networks at the end of life in Weston-super-Mare, UK
3 Compassionate Communities in Shropshire, West Midlands, England
4 Compassionate Communities in Sandwell, West Midlands, England
5 Community partnerships: a public health approach to ageing, death, dying and loss
6 The Compassionate City Charter: inviting the cultural and social sectors into end of life care
7 ‘Join Bill United!’: Compassionate Communities in Limerick, Ireland
8 Caring community in living and dying in Landeck, Tyrol, Austria
9 ‘Ethics from the bottom up’: promoting networks and participation through shared stories of care
10 Dementia-friendly pharmacy: a doorway in the community in Vienna and Lower Austria
11 A convent initiative: Compassionate Community in Solothurn, Switzerland
12 Community palliative care in Eastern Switzerland: the role of local forums in developing palliative care culture and enabling ethical discourse
13 Dementia-friendly communities: together for a better life with (and without) dementia
14 On the way to a Caring Community? The German debate
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Compassionate Communities by Klaus Wegleitner, Katharina Heimerl, Allan Kellehear, Klaus Wegleitner,Katharina Heimerl,Allan Kellehear in PDF and/or ePUB format, as well as other popular books in Social Sciences & Health Care Delivery. We have over 1.5 million books available in our catalogue for you to explore.