- 600 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Applied Respiratory Physiology
About this book
Applied Respiratory Physiology, Third Edition focuses on the applications of respiratory physiology and is designed to bridge the gap between applied respiratory physiology and the treatment of patients. This book is divided into two parts; the first of which is confined to general principles and the second deals with the various applied situations. This text is comprised of 29 chapters. After giving a general introduction to human respiratory physiology, including the functional anatomy of the respiratory tract, this book turns to the topic of the elastic resistance afforded by lungs and chest wall, along with its effect on the resting end-expiratory lung volume or functional residual capacity. The role of anesthesia in the control of breathing and the relative distribution of ventilation and perfusion are then examined. The section on artificial ventilation covers the techniques of ventilation and extracorporeal gas exchange. The reader is also introduced to special forms of lung pathology that have a major effect on lung function, including the adult respiratory distress syndrome, pulmonary oedema, embolus, and collapse. Sleep, smoking, diving, and drowning are also examined in this book. In addition, this text provides substantial coverage of exercise, high altitude, children, and neonates. This book will be of interest to clinicians and practitioners of applied respiratory physiology.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
PART I
BASIC PRINCIPLES
Outline
Chapter 1: Functional anatomy of the respiratory tract
Chapter 2: Elastic forces and lung volumes
Chapter 3: Resistance to gas flow and airway closure
Chapter 4: Control of breathing
Chapter 5: Pulmonary ventilation
Chapter 6: The pulmonary circulation
Chapter 7: Distribution of pulmonary ventilation and perfusion
Chapter 8: Diffusion and alveolar/capillary permeability
Chapter 9: Carbon dioxide
Chapter 10: Oxygen
Chapter 11: Non-respiratory functions of the lung
Chapter 1
Functional anatomy of the respiratory tract
Publisher Summary
This chapter explains the functional anatomy of the respiratory tract. The structural aspects of the function of the muscles of the mouth and pharynx are best considered in relation to a paramedian sagittal. The occlusion of the larynx is achieved in various stages ranging from whisper to speech with varying degrees of approximation of the vocal folds. The tighter occlusion can, however, be achieved for the purpose of making expulsive efforts. The trachea bifurcates asymmetrically, with the right bronchus being wider and making a smaller angle with the long axis of the trachea. It is, thus, more likely to receive foreign bodies. The main, lobar and segmental bronchi have firm cartilaginous support in their walls, U-shaped in the main bronchi but in the form of irregularly shaped and helical plates lower down. Where the cartilage is in the form of irregular plates, the bronchial muscle takes the form of helical bands that form a geodesic network. The bronchial epithelium is similar to that in the trachea, although the height of the cells gradually diminishes in the more peripheral passages until it becomes cuboidal in the bronchioles.
A clear understanding of structure is a sure foundation on which to base a study of function. This chapter is not a comprehensive account of the structure of the respiratory tract but concentrates on those aspects which are most relevant to an understanding of function.
Mouth and pharynx
Structural aspects of the function of the muscles of the mouth and pharynx are best considered in relation to a paramedian sagittal section (Figure 1.1). Part (a) shows the relaxed position with mouth slightly open and a clear airway through both mouth and nose. Part (b) shows the mouth closed with occlusion of the oral airway by approximation of tongue and palate, this being the preferred position during normal quiet breathing for all except mouth breathers. Part (c) shows forced mouth breathing, as for instance when blowing through the mouth, without pinching the nose. Note that the soft palate is arched upwards and is approximated against a band of the superior constrictor of the pharynx known as Passavant’s ridge which, together with the soft palate, forms the palatopharyngeal sphincter (Passavant, 1869; Whillis, 1930). These fibres of the superior constrictor are hypertrophied in cases of cleft palate. Note also that the orifice of the eustachian tube lies above the palatopharyngeal sphincter and the tubes can be inflated only by the subject himself when the nose is pinched.
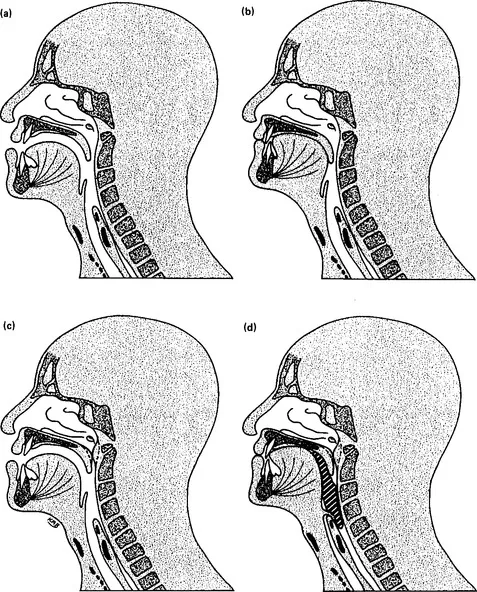
Figure 1.1 Factors in the patency of the mouth and pharynx. (a) The relaxed position with both oral and nasal airways open. (b) Oral airway occluded by the tongue, as in normal nasal breathing. (c) Nasal airway occluded at the palatopharyngeal sphincter. (d) Occlusion of the larynx and nasopharynx during swallowing. Note down-folding of the epiglottis.
Part (d) shows the occlusion of the respiratory tract during swallowing when the bolus is just passing over the back of the tongue. The larynx is elevated by contraction of the infrahyoid muscles and the epiglottis folds backwards, causing total occlusion of the entrance to the larynx (Fink and Demarest, 1978). This extremely effective protection of the larynx is capable of withstanding pharyngeal pressure as high as 80 kPa (600 mmHg) which may be generated during swallowing.
Figure 1.2 is concerned with respiratory obstruction caused by the tongue. Part (a) shows the normal position, which is substantially the same as in Figure 1.1a. The continuous lines in the body of the tongue represent the fibres of genioglossus extending from the superior genial tubercle at the symphysis menti into the body of the tongue. It is now known that this muscle has a high resting tension in the normal conscious subject and this tone shows phasic activity during the inspiratory part of the respiratory cycle (Remmers et al., 1978).

Figure 1.2 Supine position. (a) Normal relaxed position with both oral and nasal airways open. (b) Genioglossus muscle relaxed (as in coma or anaesthesia), causing obstruction between tongue and posterior pharyngeal wall. (c) Airway restored by extension of the atlanto-occipital junction. (d) Airway restored by protrusion of the mandible.
The tone in the genioglossus may be lost under certain conditions, including obstructive sleep apnoea (page 306) and almost invariably during anaesthesia (page 375). The result of this is that the relaxed tongue collapses against the posterior pharyngeal wall opposite the 2nd and 3rd cervical vertebrae, causing partial or total obstruction (Figure 1.2b).
During anaesthesia and in the comatose patient the pharyngeal airway can usually but not always be cleared by one of two manoeuvres. The simplest method, advocated for emergency resuscitation, is extension of the neck at the atlanto-occipital joint (Figure 1.2c). The effect of this has been considered in detail by Safar, Escarraga and Chang (1959). In the position shown in Figure 1.2c, the distance between the genial tubercle and the posterior pharyngeal wall is increased by about 25 per cent. The other manoeuvre to compensate for a relaxed genioglossus is protrusion of the jaw (Figure 1.2d). This is considerably more difficult and tiring to achieve but it is commonly practised by anaesthetists in patients without tracheal intubation. By this means the tongue is lifted bodily forward with the intention of clearing a passage between it and the posterior pharyngeal wall. Jaw protrusion can be combined with extension of the neck, and one or the other or both will almost always clear the airway in an unconscious patient.
Since this type of respiratory obstruction most commonly occurs in the supine position, Figure 1.2 has been drawn in that position, but it must be emphasized that gravity cannot be relied upon to solve the problem and the prone position does not usually clear a passage between tongue and posterior pharyngeal wall. It does, nevertheless, have important advantages in the clearing of secretions.
The larynx
A full account of the larynx is beyond the scope of this book and the reader is referred to Fink and Demarest (1978) for much new information on this often neglected and misunderstood organ.
Occlusion of the larynx is achieved in various stages ranging from whisper to speech with varying degrees of approximation of the vocal folds. Tighter occlusion can, however, be achieved for the purpose of making expulsive efforts. Further to simple apposition of the vocal folds and arytenoid cartilages, there is apposition of the cuneiform cartilages and vestibular folds and approximation of the thyroid cartilage and hyoid bone, with infolding of the aryepiglottic folds and apposition of the median thyrohyoid fold to the lower part of the adducted vestibular folds (Fink and Demarest, 1978). The full procedure constitutes effort clo...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Inside Front Cover
- Foreword to the First Edition
- Preface to the First Edition
- Preface to the Third Edition
- PART I: BASIC PRINCIPLES
- PART II: THE APPLICATIONS
- Appendix A: Physical quantities and units of measurement
- Appendix B: The gas laws
- Appendix C: Conversion factors for gas volumes
- Appendix D: Symbols, abbreviations and definitions
- Appendix E: Nomograms and correction charts
- Appendix F: The exponential function
- References and further reading
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Applied Respiratory Physiology by John F Nunn in PDF and/or ePUB format, as well as other popular books in Medicina & Fisiologia. We have over one million books available in our catalogue for you to explore.