eBook - ePub
Accurate Results in the Clinical Laboratory
A Guide to Error Detection and Correction
- 382 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Accurate Results in the Clinical Laboratory
A Guide to Error Detection and Correction
About this book
This practical, easy-to-use guide, named to Doody's Core Titles 2013, addresses interference issues in all laboratory tests, including patient epigenetics, process of specimen collection, enzymes, biomarkers. Clinicians and laboratory scientists can therefore rely on one reference which speaks to both their needs of accurate specimen analysis and optimal patient care.
Erroneous hospital and pathology laboratory results can be confusing and problematic, especially in acute care situations. While some factors creating interference, can be identified in the laboratory, detecting many others is often dependent on clinical details unavailable to the laboratory scientists or pathologists. Therefore, clinicians must become proficient in identifying such erroneous reports, and working with pathologists and laboratory scientists so that they can understand the source of such interferences, correct the results, and then decide what course of action must be followed for proper patient management.
- Named to Doody's Core Titles 2013, a collection development tool for health sciences libraries of all sizes, by Doody Enterprises
- Practical information for both clinicians and laboratory scientists, presented in the form of tables and charts for easy reference
- Focus on range and sources of interferences rather than details of toxicologic mechanisms which are well covered in toxicology textbooks
- Covers interferences across endocrine, oncology, hematology, immunohistochemistry, immunology, serology, microbiology, and molecular testing
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
Sciences biologiquesSubtopic
Anatomie humaine et physiologieChapter 1
Variation, Errors, and Quality in the Clinical Laboratory
Jorge Sepulveda, Columbia University Medical Center, New York, New York
Introduction
It has been roughly estimated that approximately 70% of all major clinical decisions involve consideration of laboratory results. In addition, approximately 40–94% of all objective health record data are laboratory results [1–3]. Undoubtedly, accurate test results are essential for major clinical decisions involving disease identification, classification, treatment, and monitoring. Factors that constitute an accurate laboratory result involve more than analytical accuracy and can be summarized as follows:
1. The right sample was collected on the right patient, at the correct time, with appropriate patient preparation.
2. The right technique was used collecting the sample to avoid contamination with intravenous fluids, tissue damage, prolonged venous stasis, or hemolysis.
3. The sample was properly transported to the laboratory, stored at the right temperature, processed for analysis, and analyzed in a manner that avoids artifactual changes in the measured analyte levels.
4. The analytical assay measured the concentration of the analyte corresponding to its “true” level (compared to a “gold standard” measurement) within a clinically acceptable margin of error (the total acceptable analytical error (TAAE)).
5. The report reaching the clinician contained the right result, together with interpretative information, such as a reference range and other comments, aiding clinicians in the decision-making process.
Failure at any of these steps can result in an erroneous or misleading laboratory result, sometimes with adverse outcomes. For example, interferences with point-of-care glucose testing due to treatment with maltose-containing fluids have led to failure to recognize significant hypoglycemia and to mortality or severe morbidity [4].
Errors in the Clinical Laboratory
Errors can occur in all the steps in the laboratory testing process, and such errors can be classified as follows:
1. Pre-analytical steps, encompassing the decision to test, transmission of the order to the laboratory for analysis, patient preparation and identification, sample collection, and specimen processing.
2. Analytical assay, which produces a laboratory result.
3. Post-analytical steps, involving the transmission of the laboratory data to the clinical provider, who uses the information for decision making.
Although minimization of analytical errors has been the main focus of developments in laboratory medicine, the other steps are more frequent sources of erroneous results. An analysis indicated that in the laboratory, pre-analytical errors accounted for 62% of all errors, with post-analytical representing 23% and analytical 15% of all laboratory errors [5]. The most common pre-analytical errors included incorrect order transmission (at a frequency of approximately 3% of all orders) and hemolysis (approximately 0.3% of all samples) [6]. Other frequent causes of pre-analytical errors include the following:
• Patient identification error
• Tube-filling error, empty tubes, missing tubes, or wrong sample container
• Sample contamination or collected from infusion route
• Inadequate sample temperature.
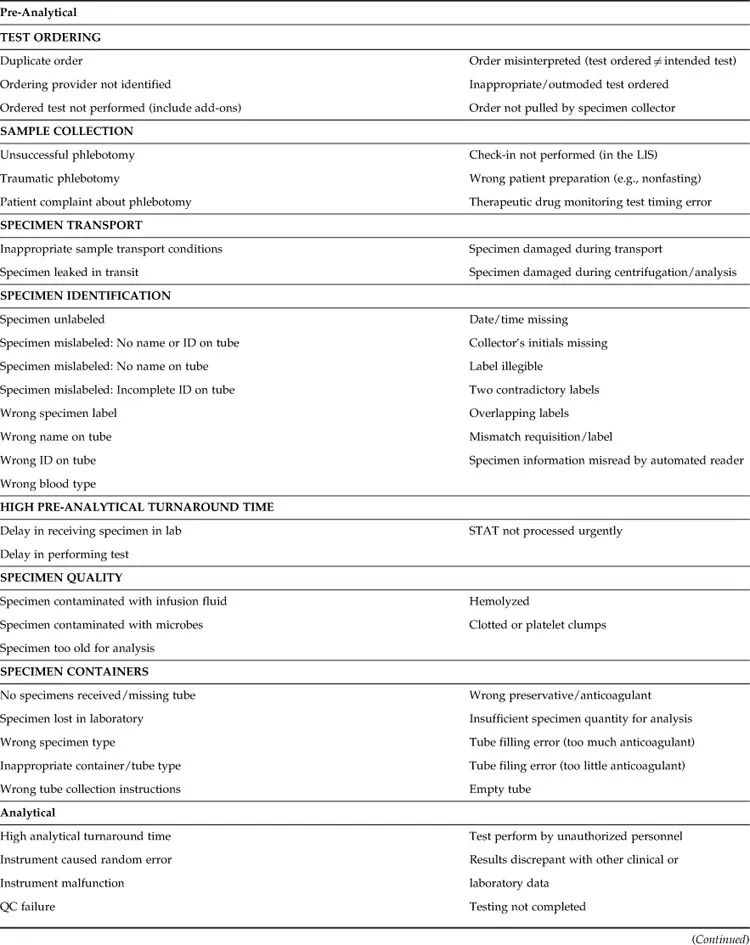
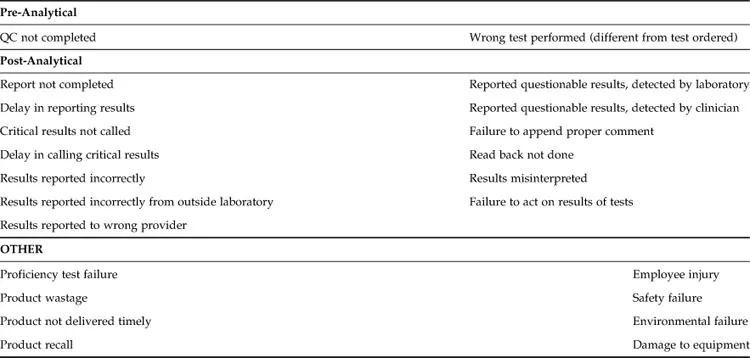
Table 1.1 provides a complete list of errors, including pre-analytical, analytical, and post-analytical errors, that may occur in clinical laboratories. Particular attention should be paid to patient identification because errors in this critical step can have severe consequences, including fatal outcomes, for example, due to transfusion reactions. To minimize identification errors, health care systems are using point-of-care identification systems, which typically involve the following:
1. Handheld devices connected to the laboratory information systems (LIS) that can objectively identify the patient by scanning a patient-attached bar code, typically a wrist band.
2. Current laboratory orders can be retrieved from the LIS.
3. Ideally, collection information, such as correct tube types, is displayed in the device.
4. Bar-coded labels are printed at the patient’s side, minimizing the possibility of misplacing the labels on the wrong patient samples.
Table 1.1
Types of Error in the Clinical Laboratory
Analytical errors are mostly due to interference or other unrecognized causes of inaccuracy, whereas instrument random errors accounted for only 2% of all laboratory errors in one study [5]. According to that study, most common post-analytical errors were due to communication breakdown between the laboratory and the clinicians, whereas only 1% were due to miscommunication within the laboratory, and 1% of the results had excessive turnaround time for reporting [5]. Post-analytical errors due to incorrect transcription of laboratory data have been greatly reduced because of the availability of automated analyzers and bidirectional interfaces with the LIS [5]. However, transcription errors and calculation errors remain a major area of concern in those testing areas without automated interfaces between the instrument and the LIS. Further developments to reduce reporting errors and minimize the testing turnaround time include autovalidation of test results falling within pre-established rule-based parameters and systems for automatic paging of critical results to providers.
When classifying sources of error, it is important to distinguish between cognitive errors, or mistakes, which are due to poor knowledge or judgment, and noncognitive errors, commonly known as slips and lapses, due to interruptions in a process that is routine or relatively automatic. Whereas the first type can be prevented by increased training, competency evaluation, and process aids such as checklists or “cheat sheets” summarizing important steps in a procedure, noncognitive errors are best addressed by process improvement and environment re-engineering to minimize distractions and fatigue. Furthermore, it is useful to classify adverse occurrences as active—that is, the immediate result of an action by the person performing a task—or as latent or system errors, which are system deficiencies due to poor design or implementation that enable or amplify active errors. In one study, only approximately 11% of the errors were cognitive, all in the pre-analytical phase, and approximately 33% of the errors were latent [5]. Therefore, the vast majority of errors are noncognitive slips and lapses performed by the personnel directly involved in the process. Importantly, 92% of the pre-analytical, 88% of analytical, and 14% of post-analytical errors were preventable. Undoubtedly, human factors, engineering, and ergonomics—optimization of systems and process redesigning to include increased automation and user-friendly, simple, and rule-based functions, alerts, barriers, and visual feedback—are more effective than education and personnel-specific solutions to consistently increase laboratory quality and minimize errors.
Immediate reporting of errors to a database accessible to all the personnel in the health care system, followed by automatic alerts to quality management personnel, is important for accurate tracking and timely correction of latent errors. In our experience, reporting is improved by using an online form that includes checkboxes for the most common types of errors together with free-text for additional information (Figure 1.1). Reviewers can subsequently classify errors as cognitive/noncognitive, latent/active, and internal to laboratory/internal to institution/external to institution; determine and classify root causes as involving human factors (e.g., communication and training or judgment), software, or physical factors (environment, instrument, hardware, etc.); and perform outcome analysis. Outcomes of errors can be classified as follows:
1. Target of error (patient, staff, visitors, or equipment).
2. Actual outcome on a severity scale (from unnoticed to fatal) and worst outcome likelihood if error was not intercepted, because many errors are corrected before they cause injury. Errors with significant outcomes or likelihoods of adverse outcomes should be discussed by quality management staff to determine appropriate corrective actions and process improvement initiatives.
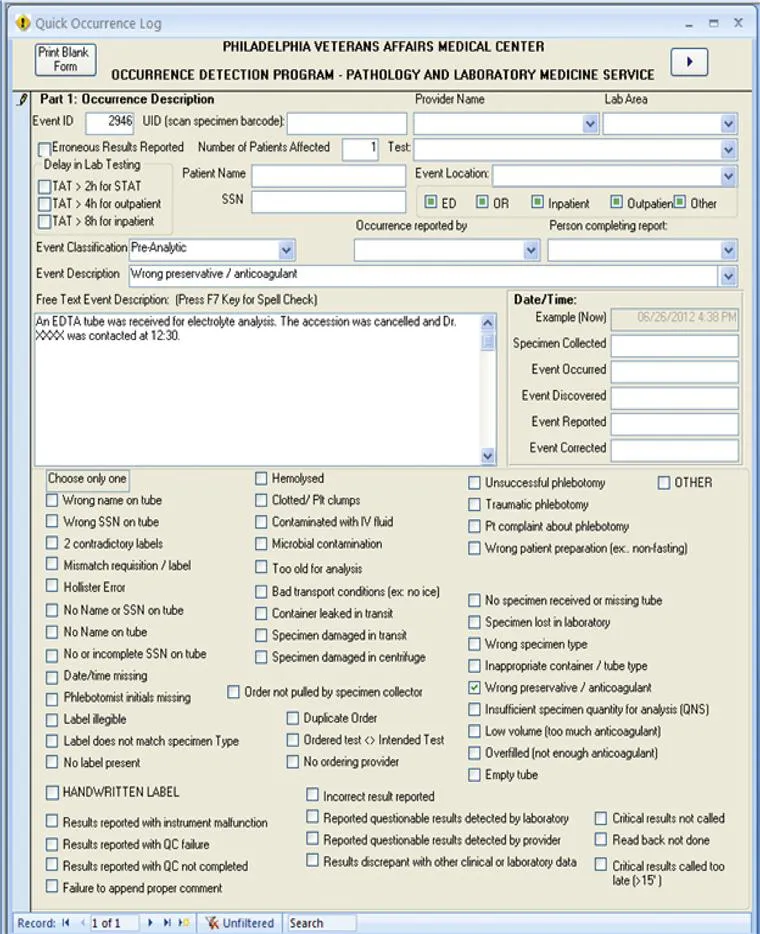
Figure 1.1 Example of an error reporting form for the clinical laboratory.
Clearly, efforts to improve accuracy of laboratory results should encompass all of the steps of the testing cycle, a concept expressed as “total testing process” or “brain-to-brain testing loop” [7]. Approaches to achieve error minimization derived from industrial processes include total quality management (TQM); [8] lean dynamics and Toyota production systems; [9] root cause analysis (RCA); [10] health care failure modes and effects analysis (HFMEA); [11,12] failure review analysis and corrective action system (FRACAS) [13]; and Six Sigma [14,15], which aims at minimizing the variability of products such that the statistical frequency of errors is below 3.4 per million. A detailed description of these approaches is beyond the scope of this book, but laboratorians and quality management specialists should be familiar with these principles for efficient, high-quality laboratory operation [8].
Quality Improvement in the Clinical Laboratory
Quality is defined as all the features of a product that meet the requirements of the customers and the health care system. Many approaches are used to improve and ensure the quality of laboratory operations. The concept of TQM involves a ph...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Foreword
- Preface
- List of Contributors
- Chapter 1. Variation, Errors, and Quality in the Clinical Laboratory
- Chapter 2. Effect of Age, Gender, Diet, Exercise, and Ethnicity on Laboratory Test Results
- Chapter 3. Effect of Patient Preparation, Specimen Collection, Anticoagulants, and Preservatives on Laboratory Test Results
- Chapter 4. Sample Processing and Specimen Misidentification Issues
- Chapter 5. Hemolysis, Lipemia, and High Bilirubin: Effect on Laboratory Tests
- Chapter 6. Immunoassay Design and Mechanisms of Interferences
- Chapter 7. Effect of Herbal Remedies on Clinical Laboratory Tests
- Chapter 8. Challenges in Routine Clinical Chemistry Testing: Analysis of Small Molecules
- Chapter 9. Challenges in Routine Clinical Chemistry Analysis: Proteins and Enzymes
- Chapter 10. Sources of Inaccuracy in Biochemical Genetics Testing
- Chapter 11. Challenges in Endocrinology Testing
- Chapter 12. Pitfalls in Tumor Markers Testing
- Chapter 13. Issues of Interferences in Therapeutic Drug Monitoring
- Chapter 14. Limitations of Drugs of Abuse Testing
- Chapter 15. Challenges in Confirmation Testing for Drugs of Abuse
- Chapter 16. Alcohol Determination Using Automated Analyzers: Limitations and Pitfalls
- Chapter 17. Pre-Analytical Issues and Interferences in Transfusion Medicine Tests
- Chapter 18. Issues with Immunology and Serology Testing
- Chapter 19. Sources of Errors in Hematology and Coagulation Testing
- Chapter 20. Challenges in Clinical Microbiology Testing
- Chapter 21. Sources of Errors in Molecular Testing
- Chapter 22. Problems in Pharmacogenomics Testing
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Accurate Results in the Clinical Laboratory by Amitava Dasgupta,Jorge L. Sepulveda in PDF and/or ePUB format, as well as other popular books in Sciences biologiques & Anatomie humaine et physiologie. We have over 1.5 million books available in our catalogue for you to explore.