eBook - ePub
The Plasticity of Sex
The Molecular Biology and Clinical Features of Genomic Sex, Gender Identity and Sexual Behavior
- 318 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The Plasticity of Sex
The Molecular Biology and Clinical Features of Genomic Sex, Gender Identity and Sexual Behavior
About this book
The Plasticity of Sex: The Molecular Biology and Clinical Features of Genomic Sex, Gender Identity and Sexual Behavior provides a comprehensive view on the development of human sexuality. As there has been a crescendo of interest over the past several decades about the nature and diversity of human sexuality, this reference brings the evidence-based research into one place. The emergence of issues surrounding gender identity, genital ambivalence and the transition from one sex to another is striking, with the public and treating physicians alike clamoring for an evidence-based, comprehensive treatment of human sexuality and all its variations.
This is a must-have reference for biomedical researchers in endocrinology, neuroscience, development biology, medical students, residents, and practicing physicians from all medical areas.
Winner of the 2021 PROSE Award in Biomedicine from the Association of American Publishers!
- 2021 PROSE Awards - Winner: Category: Biomedicine: Association of American Publishers
- Discusses the role of biology in gender identity from research in genetics, endocrinology and neuroscience
- Addresses important health disparities and how to address them when treating the transgender patient
- Reviews evidence-based information on the biological basis and impact of environmental and hormonal factors at different life stages
- Outlines schema for treating variations in the sexuality and sexual function of the individual patient
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Endocrinology & MetabolismChapter 1
What determines biological sex?
Marianne J. Legato1, 2, 1Department of Medicine, Columbia University, New York, NY, United States, 2Department of Medicine, Johns Hopkins University, Baltimore, MD, United States
Abstract
The X and Y chromosomes establish biological sex, have a unique pattern of interaction, and are established in the haploid male and female gametes through the specialized process of cell replication called meiosis. Meiosis generates zygotes with randomly distributed chromosomes, guaranteeing the potential for extensive variation in the embryonic phenotype. In the process of replication, epimarks that regulate gene activity are erased and reestablished in a pattern reflecting the sex of the zygote. The features of the two chromosomes vary significantly; the X has over a thousand genes—5% of the total genes in the human genome. The Y’s ability to establish male sex is jealously guarded by protection from recombination with the X along a significant portion of the chromosome. The nascent gonad is neutral and composed of both germ and somatic cells that are bipotential; they have the unique property of being capable of differentiating into either a female or male lineage. The two different pathways are regulated by the complex interaction of and balance between genes that function in the first phases of gonadal development.
Keywords
Biological sex; mitotic process; meiosis; male and female gametes; gametocyte; mtDNA
Most adult mammals exhibit clear sexual dimorphism that manifests externally and internally.1
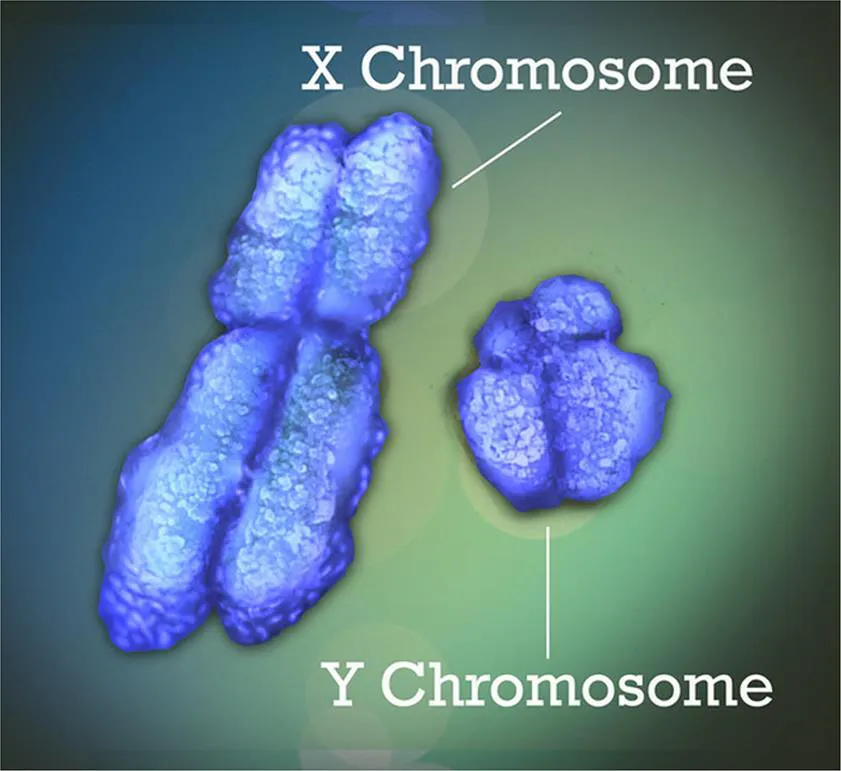
The X and Y chromosomes are arguably the most fascinating members of the human genome: they determine biological sex. The XX combination produces a female and the XY a male. These chromosomes have a unique pattern of interaction compared with autosomes and in a specialized process of duplication called meiosis, produce gametes which are the source of a virtually infinite series of variations in gene content.

1.1 Cell multiplication and the mechanisms of heredity
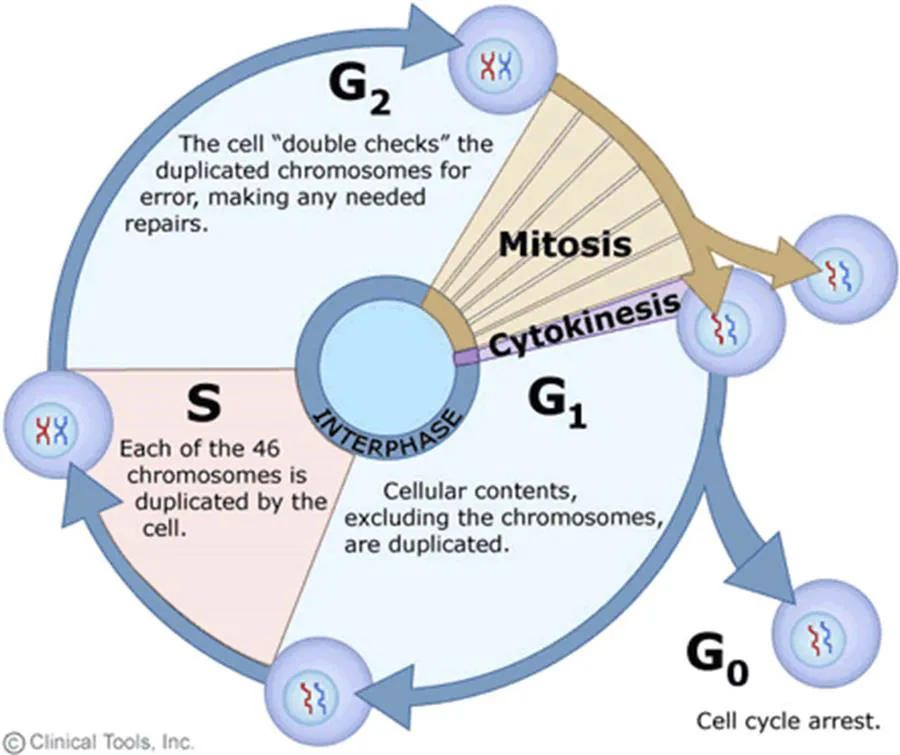
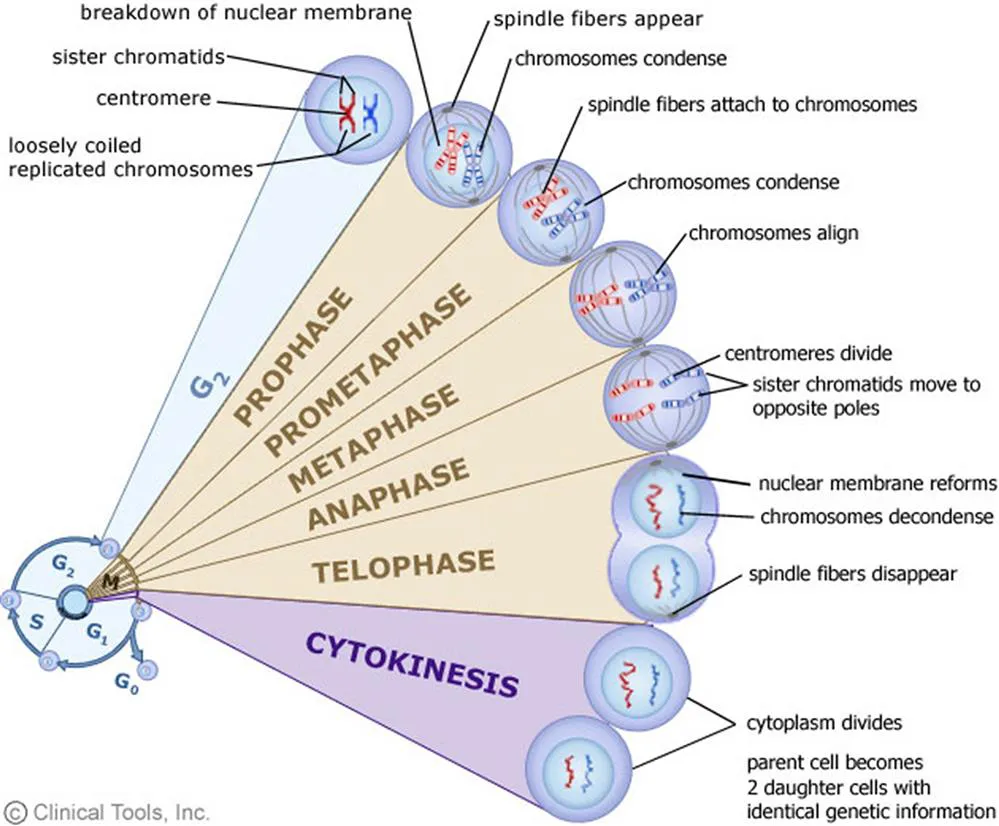
1.1.1 Mitosis
The mitotic process is the method in which cells produce two identical copies of themselves. It is responsible for the organism’s normal growth and the maintenance of tissue. Mitosis begins with a duplication of each chromosome into two sister chromatids in anticipation of the distribution of these chromatids into daughter cells. Each DNA molecular pair in a chromosome is “unzipped” and copied. The duplicated DNA is distributed to each of an identical pair, called sister chromatids. These will separate and each will ultimately be transmitted to a daughter cell, identical in chromosome number and composition to the parent cell. Mitosis is essential for normal growth and tissue repair/regeneration.
A failure of chromatids or autologous chromosomes to separate in cellular fission is called nondisjunction: one daughter cell gets NO copy of the original chromosome and the other gets TWO. The three most common examples in children that survive include Down’s syndrome, in which the zygote has an extra copy of chromosome 21: two from the mother and one from the father. This phenomenon of trisomy is reproduced in all the somatic cells. The rate of nondisjunction increases with age, which is why the chances for Down’s syndrome increase between 35 and 45, going from 1 in 350 at age 35 to 1 in 10 at 45. Other examples of trisomy are Trisomy 13 (Patau syndrome) in which there are three copies of chromosome 13 causing intellectual impairment and many physical abnormalities.2 Edward’s syndrome is an extra chromosome 18 which occurs in about 1 in 2500 pregnancies and 1 in 6000 live births.3
1.1.2 Meiosis
In contrast to the mitotic process the sequence of events that produces the sexual gamete (either a sperm or an ovum) begins in the process of meiosis.4 Meiosis is a system unique to the production of male and female gametes. Meiosis generates four gametes from a single primordial germ cell each of which contains half the number of the full complement of chromosomes (haploid) so that when fertilization occurs, the resulting zygote has the full complement of 46 chromosomes—half from each of its two parents. This reduction of the number of chromosomes is achieved in two sequential processes known as meiosis 1 and meiosis 2.

The enormous variety of genetic composition in each of the gametes creates the advantage of sexual reproduction and ensures a potentially almost infinite diversity of traits in the phenotype. This is achieved in two stages: the first is the result in the first cell division (meiosis 1) of an extensive exchange of DNA between tightly connected autologous chromosomes (one from each parent) prompted by a programmed induction of DNA double-strand breaks, in the phenomenon called crossover. The distribution of the sites of these breaks is not random but is controlled by PR domain-containing 9 (PRDM9).5 This system avoids the targeting of basic regulatory elements in the DNA strand. There are also newly identified partners in the process of coordinating and regulating the crossover and noncrossover pathways; the significance of noncrossover pathways has not yet been completely elucidated.
The second meiotic cell division (meiosis 2) further promotes genetic variation when the newly constituted chromosomes are randomly arranged into two groups. These are separated in turn and delivered to two new cells, called haploid gametocytes. In males, this results in two secondary spermatocytes, but in females, a large secondary oocyte and a much smaller polar body are produced. [Importantly, in spite of its significantly smaller compliment of cytoplasm, the polar body contains all the genetic material (both chromosomal and mitochondrial) of the parent gametocyte. Each polar body continues to meiotically divide.]
In females, meiosis I is initiated synchronously in all the cells of the fetal ovaries early in development, producing secondary oocytes, but is arrested after birth until a second meiotic division (meiosis 2) resumes in selected primary oocytes after puberty. In males the first and second meiotic divisions go on in an unbroken sequence throughout reproductive life; each primordial germ cell produces four haploid spermatids. In females the second meiotic division occurs after fertilization; the fertilized egg contains two haploid pronuclei (one from the father and the other from the mother) and three haploid polar bodies.

The polar body is of special interest because like its larger sister cell, the polar body contains—and is a potential source of—the entire compliment of both chromosomal and mitochondrial DNA; thus it has several potential uses. Ma et al. describe the generation of functional human oocytes, for example, following the injection of polar body genomes from metaphase II oocytes into enucleated donor cytoplasm.6 This is an important contribution to the treatment of infertility; current assisted reproductive techniques are limited by the number and quality of oocytes, which decline as women age; similarly, the time to conception and the likelihood of miscarriage increase as women grow older. Leridon, writing in 2004, commented that all the then available techniques for assisted reproduction could not compensate for the natural decline of fertility after age 35.7 Similarly, polar bodies have the capacity for mitochondrial-replacement therapy to prevent transmission to a subsequent generation of mitochondrial DNA (mtDNA) disease.8 When mitochondrial mutation is over 60%, progeny may develop severe systemic disease, such as myopathies, neurodegenerative diseases, diabetes, cancer, and infertility. Wang comments, “currently, inherited mitochondrial diseases are incurable and the treatments available are predominantly supportive.” Although mtDNA contains only 37 genes, over 700 mutations in mtDNA have been identified.9 Wolf et al. discuss the possibility of mitochondrial-replacement therapies in oocytes or zygotes to prevent second-generation transmission of mtDNA defects.10 Finally, Verlinsky et al. have demonstrated the feasibility of performing preconception genetic analysis by the removal and analysis of the first polar body, which bypasses the need to biopsy preembryonic or extraembryonic cells and allows embryo transfer without the need for cryopreservation required for blastomere biopsy at the eight cell stage.11
Meiosis in the male involves an additional phenomenon, meiotic sex chromosome inactivation. This silencing the X component of the male germ cell as it enters meiosis protects against aneuploidy in subsequent generations.12 (Even this process is not clear-cut; some genes on the silenced X may escape inactivation.)
Primary gametocytes of both sexes have chromosomes composed of two sister chromatids. However, the timing of entry into meiosis is not the same for the two sexes. As we have said, female oocytes enter meiosis 1 in a completely synchronized fashion toward the last part of embryogenesis. The meiotic process is halted then until puberty, when oocytes enter meiosi...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- List of contributors
- Foreword
- Introduction
- Chapter 1. What determines biological sex?
- Chapter 2. Disorders of sex development
- Chapter 3. The sexual brain
- Chapter 4. The transgender individual
- Chapter 5. Homosexuality: the biological basis of differences in sexual orientation
- Chapter 6. The strong heritability of gender dysphoria
- Chapter 7. 5α-Reductase deficiency syndrome: the impact of androgens on gender identity and gender role
- Chapter 8. Biological basis of gender identity
- Chapter 9. Congenital adrenal hyperplasia as a model to explore gender fluidity in early life; particularly 46,XX patients with male external genitalia
- Chapter 10. Testosterone treatment for transgender (trans) men
- Chapter 11. Transgender care
- Chapter 12. Fertility preservation for transgender individuals
- Chapter 13. Breast imaging in transgender individuals
- Chapter 14. Protecting children with intersex traits: legal, ethical, and human rights considerations
- Chapter 15. Transphobic discrimination and health
- Chapter 16. Societal experiences of lesbian, gay, bisexual, and transgender people
- Chapter 17. Implementing LGBTQ curricula into health professions education
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Plasticity of Sex by Marianne Legato J,Marianne J. Legato in PDF and/or ePUB format, as well as other popular books in Medicine & Endocrinology & Metabolism. We have over 1.5 million books available in our catalogue for you to explore.