- 326 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Advances in research have led to the use of robotics in a range of surgical applications. Medical robotics: Minimally invasive surgery provides authoritative coverage of the core principles, applications and future potential of this enabling technology.Beginning with an introduction to robot-assisted minimally invasive surgery (MIS), the core technologies of the field are discussed, including localization and tracking technologies for medical robotics. Key applications of robotics in laparoscopy, neurology, cardiovascular interventions, urology and orthopaedics are considered, as well as applications for ear, nose and throat (ENT) surgery, vitreoretinal surgery and natural orifice transluminal endoscopic surgery (NOTES). Microscale mobile robots for the circulatory system and mesoscale robots for the gastrointestinal tract are investigated, as is MRI-based navigation for in vivo magnetic microrobots. Finally, the book concludes with a discussion of ethical issues related to the use of robotics in surgery.With its distinguished editor and international team of expert contributors, Medical robotics: Minimally invasive surgery is a comprehensive guide for all those working in the research, design, development and application of medical robotics for surgery. It also provides an authoritative introduction for academics and medical practitioners working in this field.
- Provides authoritative coverage of the core principles, applications and future potential of medical robotics
- Introduces robot-assisted minimally invasive surgery (MIS), including the core technologies of the field and localization and tracking technologies for medical robotics
- Considers key applications of robotics in laparoscopy, neurology, cardiovascular interventions, urology and orthopaedics
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Introduction to robot-assisted minimally invasive surgery (MIS)
V. Vitiello, K.-W. Kwok and G.-Z. Yang, The Hamlyn Centre for Robotic Surgery, Imperial College London, UK
Abstract:
It is well recognised that the performance of minimally invasive surgery (MIS) imposes an increasing burden on surgeons’ manual dexterity and visuomotor control. Tissue deformation, restricted workspace, and a limited field-of-view make manual operation of the procedure difficult. With the advent of robot assisted MIS, manual dexterity is enhanced by microprocessor controlled mechanical wrists, allowing motion scaling and tremor removal. Further enhancement of three-dimensional (3D) vision and intra-operative image guidance permits improved clinical uptake of the technology, ensuring better operative safety and consistency. This chapter provides a detailed overview of robotic surgical systems and introduces recent developments in the integration of synergistic controls such as virtual fixtures, dynamic active constraints, and perceptual docking.
Key words
minimally invasive surgery
medical robotics
robot-assisted surgery
virtual fixtures
perceptual docking
1.1 Introduction
In the past few decades, surgical practice has been revolutionised by the introduction of advanced instrumentation enabling a paradigm shift from traditional open surgery to minimally invasive surgery (MIS). The main advantage of MIS is attributed to a reduction in patient trauma, resulting in faster recovery and lower hospitalisation costs. However, the very nature of MIS, laparoscopy for example, which involves the use of long, rigid tools inserted into the patient via small incisions, can introduce a range of ergonomic challenges. The loss of wrist articulation together with the fulcrum effect caused by the inversion of motion direction at the trocar, limits the manual dexterity of the surgeon. In addition, the use of a separate display to convey the visual feedback from a laparoscopic camera separates the visuomotor axes, thus affecting the hand-eye coordination of the surgeon (Howe and Matsuoka, 1999).
Improved control and dexterity is one of the main benefits of robotic technologies for MIS. Mechatronically enhanced surgical instruments have been designed to compensate for the loss of wrist articulation caused by the traditional approach. Together with the introduction of master–slave control, this has contributed to the safety and consistency of MIS (Camarillo et al., 2004). However, even with the current state-of-the-art robotic surgical systems, such as the da Vinci from Intuitive Surgical Inc. (Guthart and Salisbury, 2000), tools are still rigid and require careful port placement to ensure required access and workspace for a given procedure. Safe performance of surgical interventions within the tight confines of the chest or cluttered peritoneal cavity involving large-scale tissue deformation is a significant challenge. Current medical robotics research is therefore focused on the integration of multiple control modalities such as perceptual docking and virtual fixtures together with enhanced visualisation and intraoperative image guidance.
Historically, most initial research in medical robotics has been directed to overcoming known limitations of industrial robots, particularly in terms of adaptability and autonomy. The main perceptual differences between humans and robots lie in the ability of processing qualitative and quantitative information. Robots can integrate a large amount of quantitative data precisely through different sensors, thus being able to perform and repeat repetitive tasks with good stability and positional accuracy. On the other hand, surgeons are superior in combining diverse sources of qualitative information for making difficult decisions. Such skills are critical to the success of any surgical intervention, but existing surgical robots are still limited to simple procedures under the direct control of surgeons. Unlike industrial automation, robotic systems for surgery must be considered as a ‘surgeon’s extender’ rather than a ‘surgeon’s replacement’ (Camarillo et al., 2004; Howe and Matsuoka, 1999).
It is important to note that robotic-assisted surgery is only one of the various specialties falling under the broader category of computer-aided surgery (CAS). In this context, the robot represents a single component of a multifunctional system specifically designed to augment the capabilities of surgeons and to improve the overall outcome of surgical procedures. Through a combined use of automated and manually controlled surgical devices, such a system also incorporates preoperative planning, intraoperative registration, and image-guided navigation and visualisation (Taylor and Stoianovici, 2003). In this regard, medical imaging plays a fundamental role in the development of CAS systems and there is a unique opportunity in combining the two. To better understand the benefits and technical challenges of robot-assisted MIS, this chapter provides a detailed overview of robotic surgical systems and introduces recent developments in the integration of multiple control modalities such as perceptual docking and virtual fixtures.
1.2 Minimally invasive surgery and robotic integration
During MIS, a set of three to five incisions of about 1 cm length is usually required to introduce at least two long-handled tissue manipulators, such as grippers and retractors, and one video endoscope to visualise the operative site, as shown in Fig. 1.1a. The main advantages of MIS are related to reduced tissue scar and surgical trauma, less pain and faster recovery (Howe and Matsuoka, 1999). However, the particular configuration of MIS instrumentation also imposes substantial limitations on manual manipulation and hand–eye coordination (Camarillo et al., 2004). The use of rigid, long hand-held tools can result in a loss of surgeon’s wrist articulation, while the fixed access port can constrain the lateral movements of the instrument shaft, acting like a fulcrum or remote centre of motion (RCM). The direction of surgeon’s hand motion is therefore reversed at the instrument tip and motion is scaled depending on the relative position of the tool to the trocar, as shown in Fig. 1.1b.
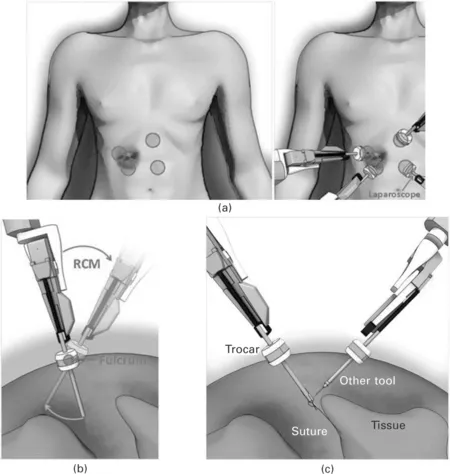
Fig 1.1 (a) A typical port arrangement for laparoscopic surgery: (left) four circles indicate the approximate locations of incision points for laparoscopic cholecystectomy; (right) four manipulators holding the instruments and a laparoscope are required to share a small workspace inside the abdominal cavity. (b) An illustration of the fulcrum effect and RCM at the fulcrum point. (c) Possible forces applied by the trocar, suture, tissue and other tool on the laparoscopic instrument on the left.
In addition to the fulcrum effect, indirect vision of the operative area through a two-dimensional (2-D) display, often located away from the surgeon, presents an unfamiliar relationship between visual and motor coordinates. Furthermore, the field-of-view is often limited by the use of an endoscopic camera, and the view angle can be unnatural because of the constrained position and orientation of the tool. Finally, the perceptual capabilities of the surgeon are also affected by a lack of tactile sensation and force feedback. During surgery, the instruments are interacting with many objects such as the trocar, tissue or other instruments, as shown in Fig. 1.1c. The use of long, rigid shafts significantly affects force perception at the instrument tip and can lead to undesired damage caused by excessive forces applied on the tissue.
The application of robotic technologies to MiS is aimed at solving many of these drawbacks (Mack, 2001). Recent advances in imaging such as three-dimensional (3-D) wide-angle endoscopic cameras and high-resolution stereoscopic displays have already been incorporated into the current robotic surgical systems (Ballantyne and Moll, 2003). Structural and functional imaging modalities have been integrated for improved tissue characterisation and additional navigational clues (Noonan et al., 2009). the articulated tools incorporate an additional degree of dexterity to allow for improved flexibility and manual dexterity (Low and Phee, 2004; Noonan et al., 2009).
Thus far, much effort has been devoted to the development of teleoperated surgical systems based on one or more robotic slave manipulators at the patient side controlled by the surgeon through a master console that can be remotely located (Low and Phee, 2004). The surgeon can benefit from visual and sometimes haptic feedback at the master console, and highly dexterous slave manipulators. Hand tremor elimination and motion scaling are provided to obtain accurate movements, as well as improved ergonomics and visuomotor integration. Some robotic systems, such as the da Vinci can be used for a range of surgical tasks, whereas others are designed for specific surgical tasks. there are also systems that exploit the stability and geometric accuracy of robots to perform microscopic surgical procedures (taylor et al., 1999) or for replacing surgical assistants for tasks such as endoscope positioning (Sackier and Wang, 1994) and organ retraction (Osaki et al., 2009). A summary of the drawbacks associated with traditional MIS and the corresponding benefits of robotic integration is presented in Table 1.1
Table 1.1
Summary of MIS drawbacks and related benefits of robotic integration

© 2009 Intuitive Surgical Inc.
1.3 Definitions and development of surgical robotic systems
In the literature, several authors have attempted to classify surgical robotic systems developed in the last 25 years into specific categories (Camarillo et al., 2004; Cleary and Nguyen, 2001; Dario et al., 2003; Davies, 2000; Howe and Matsuoka, 1999; Taylor and Stoianovici, 2003). According to Taylor (Taylor, 1997), these can be based on three main criteria: the interaction mode between the robot and the surgeon, the clinical application, and the role played by the robot during surgical procedures. Systems are defined by the first criterion depending on the level of autonomy of the robot, ranging from autonomous to master-slave systems (Dario et al., 2003; Davies, 2000). application-ba...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Contributor contact details
- Dedication
- Woodhead Publishing Series in Biomaterials
- Introduction
- Chapter 1: Introduction to robot-assisted minimally invasive surgery (MIS)
- Chapter 2: Localization and tracking technologies for medical robotics
- Chapter 3: Robotics for neurosurgery
- Chapter 4: Robotic systems for cardiovascular interventions
- Chapter 5: Robotics in orthopaedic surgery
- Chapter 6: Robotic-assisted knee replacement surgery
- Chapter 7: Robotics in ear, nose and throat (ENT) surgery
- Chapter 8: Robot-assisted vitreoretinal surgery
- Chapter 9: Robotics for minimally invasive surgery (MIS) and natural orifice transluminal endoscopic surgery (NOTES)
- Chapter 10: Mesoscale mobile robots for gastrointestinal minimally invasive surgery (MIS)
- Chapter 11: Real-time software platform using MRI for in vivo navigation of magnetic microrobots
- Chapter 12: Robotic surgery and ethical challenges
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Medical Robotics by Paula Gomes in PDF and/or ePUB format, as well as other popular books in Computer Science & Artificial Intelligence (AI) & Semantics. We have over 1.5 million books available in our catalogue for you to explore.