![]()
Part I. Epidemiological and biological issues in HIV prevention
![]()
Chapter 1. Current and futuretrends - implicationsfor HIV prevention
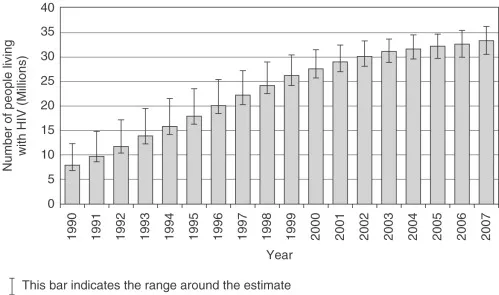
In November 2007, the Joint United Nations Program on HIV/AIDS (UNAIDS) and the World Health Organization (WHO) revised downward the estimates of the number of persons with HIV/AIDS worldwide, based on more accurate data from revised estimates in India and Africa. Their 2007 AIDS Epidemic Update estimates that of the 33.2 million (likely range: 30.6–36.1 million) persons who were living with HIV/AIDS in 2007, 30.8 million were adolescents and adults (28.2–33.6 million) and 2.5 million children <15 years of age (2.2–2.6 million)(UNAIDS, 2007; Figure 1.1). Almost half of the persons living with HIV/AIDS (PLWHA) were women: 15.4 million (13.9–16.6 million). Sub-Saharan Africa, both historically and currently, bears 68 percent of the world's disease burden while only hosting about 12 percent of the world's population. With a huge epidemic in the general population, sub-Saharan Africas HIV epidemic contrasts with the rest of the world that sees HIV heavily 'over-represented in high-risk subgroups. Sex workers and their sexual partners are over-represented as a high-risk subgroup in Asia as well as most parts of Africa, men who have sex with men (MSM) are a predominant high-risk subgroup in the HIV epidemics in the Americas, Western Europe and Australia/New Zealand, while injecting drug users (IDUs) drive the epidemic in China, southeast Asia and Eastern Europe.
Figure 1.1. Trends in the estimates of numbers of HIV-infected persons living worldwide. Source: UNAIDS (2007).
The latest epidemic trend analysis suggests that the global AIDS epidemic peaked around the turn of the century (2000–2001) (Chin, 2007; UNAIDS, 2007; Figure 1.2). Slight downward trends in new cases have been observed in many countries since 2002; some observers suggest that this is due to saturation of the highest-risk pool of individuals along with death of infected persons, while others attribute declines to slow and sporadic yet widespread successes in public health prevention programs that have reduced high-risk behaviors (Meda et al., 1999; Ainsworth et al., 2003; Shelton et al., 2006; Chin, 2007; Gregson et al., 2007). The truth is likely a mix of these factors, with differential impacts of each in different venues. AIDS mortality is also decreasing in many countries, most significantly due to improved access to antiretroviral therapy for PLWHA (Ventelou et al., 2008).
Figure 1.2. Trends in the estimates of numbers of people newly infected with HIV worldwideSource: UNAIDS (2007).
Estimates and projections: methodology and refinements
Case definitions and surveillance methodology have undergone significant revisions over the past 27 years since HIV was first described, partly as a result of improved scientific understanding of the biomedical aspects of the disease but also due to more robust population estimation methods (Schmidt and Mokotoff, 2003; Cleland et al., 2004; Posner et al., 2004; Chin, 2007). The Bangui definition by the WHO in 1986 and the United States Centers for Disease Control and Prevention (CDC)-led AIDS surveillance case definitions in 1985, 1987 and 1993 have been the backbone of AIDS case reporting based on HIV test results, clinical indications and, usually, CD4+ T cell counts (WHO, 1985; CDC, 1987, 1992). Given the reluctance of many to obtain HIV tests, and owing to the undercapacity of clinical infrastructures in developing countries, there has been significant under-reporting of AIDS cases at regional and national levels, particularly in resource-limited settings (Chin, 2007).
Population-based unlinked anonymous testing (UAT) methods have been adopted for estimating national figures. UAT has been most widely undertaken for surveillance of “sentinel” populations of pregnant women in antenatal care (ANC) clinics. This method, in use since 1989, has been applied widely, since it is operationally uncomplicated, cost-effective, sustainable, and thought to represent the general population in the most at-risk reproductive age groups. Unfortunately, this method has been shown to systematically over-represent the population HIV prevalence, since most sentinel sites have been concentrated in larger cities, under-representing rural areas. ANC clinic sampling that systematically over-samples urban women, including high-risk groups, will over-estimate population HIV seroprevalence (Saphonn et al., 2002; Dandona et al., 2006; Chin, 2007). An improved surveillance method employed in recent years by national governments includes population-based sampling and HIV-testing through Demographic and Health Surveys (DHS) (Mills et al., 2004). These estimates are significantly lower (between half to one-third) than those of the UNAIDS-promoted sentinel surveillance system. While a population-based survey is subject to bias due to under-representation (particularly for men, due to low-response rates or absenteeism), it is nonetheless more representative of the general population for estimation of national disease prevalence (Chin, 2007). “Triangulation” of multiple approaches (e.g., DHS, ANC and targeted surveys of high-risk groups) is useful to estimate most accurately the overall seroprevalence in a given venue (Bennett et al., 2006).
The culmination of this process by UNAIDS and the WHO incorporated the results of population-based surveys with sentinel surveillance data in its annual report for 2007, resulting in a substantial downward revision of the world's total numbers of persons estimated to be living with and to have died due to HIV/AIDS. In India, for example, lower than anticipated rural prevalence estimates resulted in PLWHA estimates reduced from 5.2 million to 2.5 million; similar downward revisions were made in such nations as Angola, Kenya, Mozambique, Nigeria and Zimbabwe (Dandona and Dandona, 2007; Shelton, 2007). Greater reliance on population-based surveys was accompanied by other methodological improvements in 2007, including improved HIV sentinel surveillance, expansion to more sites in relevant countries, as well as adjustments to mathematical models to accommodate a better understanding of the natural history of untreated HIV infection in low- and middle-income countries. Continuous revisions of prevalence estimates are made by UNAIDS and WHO as more data become available.
While HIV prevalence provides a snapshot of the magnitude of the pandemic, especially when accompanied by CD4+ cell-count distributions in the case of HIV surveillance, a critical indicator is the incidence of HIV infection. HIV incidence represents the number of new HIV infections in a population-at-risk per year, and can help distinguish ...