eBook - ePub
Alzheimer's Disease
Life Course Perspectives on Risk Reduction
- 466 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Alzheimer's Disease: Lifecourse Perspectives on Risk Reduction summarizes the growing body of knowledge on the distribution and causes of Alzheimer's disease (AD) in human populations, providing the reader with knowledge on how we define the disease and what its risk and protective factors are in the context of a life-course approach.
At the conclusion of the book, the reader will understand why Alzheimer's disease likely begins at conception, then progresses through early-life and adult risk factors that ultimately impact the balance between pathologic insults in the brain and the ability of the brain to modify disease symptoms. In contrast to edited volumes that may have little cohesion, this book focuses on an integrated life-course approach to the epidemiology of dementia, in particular, Alzheimer's disease.
- Reviews the current science surrounding Alzheimer's disease
- Provides a primer of foundational knowledge on the disease's epidemiology and biostatistics
- Utilizes a life-course approach, providing a novel and integrated view of the evolution of this illness from genes to brain reserve
- Uses the 'threshold model'—a theory first described by Dr. Mortimer and widely accepted today—which incorporates the idea of risk factors for the pathology and expression of the disease
- Proposes that improving brain health through modifiable behaviors can delay disease onset until a later age
- Examines the future of prevention of Alzheimer's disease, a subject of great current interest
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Section III
Analytic Epidemiology
Outline
Chapter 9
Introduction to the Analytic Epidemiology of Alzheimer’s Disease
Abstract
Effective prevention of Alzheimer’s disease (AD) will require identification of people at risk of this illness, preferably long before the first clinical symptoms. Although imaging and analysis of CSF proteins can identify individuals who will get this illness up to 15 years prior to its onset, these modalities are unlikely to be useful in populations, where the search for noninvasive, cost-effective markers is underway. Two major types of risk factors for AD can be identified, those for its pathology and those for its clinical expression. A third type of risk factor is a marker for the underlying disease. In addition to finding pharmacologic interventions that slow the pathogenesis of the disease, we need to focus on modifiable risk factors that influence its expression. Observational studies have included case–control studies that offered the first clues to risk factors and cohort studies. Both of these types of studies have associated methodological problems and the accepted hierarchy of study designs with randomized controlled trials at the top followed by cohort studies and then by case–control studies needs to be reconsidered in studies of Alzheimer’s disease.
Keywords
Prevention; risk factors; biomarkers; case–control studies; cohort studies; methodology
When biologically modifying drugs become available to treat Alzheimer’s disease (AD), these medications are likely to be most effective if given to people in the preclinical phase of the illness. Discovering who these at-risk people are is best approached using a multimodal strategy, including epidemiologic risk factors and markers, genetic markers, neuropsychological testing, imaging, and cerebrospinal fluid or blood markers.
Because we are interested in preventing AD in the general population, the methodology for identifying preclinical cases of the disease must be both cost-effective and acceptable. It is unlikely that we can afford to give everyone every test to detect AD early, even if they were to agree to a prolonged and often invasive set of measures. Therefore, we will need to prioritize markers to those with sufficiently high sensitivity and specificity that are both cost effective and acceptable.
Preventing the disease is an alternative option to “curing” the disease. Currently, funding for prevention represents a tiny fraction of the monies that have been invested in trying to find a cure. One estimate from the United Kingdom cites that ratio as 1 penny:1,000 pounds (D. Smith, 2013). Clinical trials of drugs to treat AD have generally failed, except for cholinesterase inhibitors and memantine (for an excellent review, see L. S. Schneider, Mangialasche, et al., 2014).
It is our view that we do not have to wait until an effective drug is developed to begin preventing AD. For example, there is abundant evidence that cardiovascular risk factors are associated with increased risk for AD and that physical and mental exercise as well as nutritional factors can influence its development. Most of these data come from observational studies, which represent the long-term effects of chronic exposures over the life course in a disease that develops over decades. In addition, a small number of clinical trials have been performed, showing that nutritional as well as physical and mental exercise interventions can influence the shrinkage of the brain that is related to AD expression. The remainder of this book will discuss factors that either increase the risk for AD or are inversely associated with this risk. Both observational and experimental studies will be considered. Again, our focus is not to include every study that has been conducted, but to give a critical and updated view of each risk or protective factor within the context of the best studies.
In 2004, we proposed that there are two major types of risk factors for AD (Borenstein Graves, 2004). The first type refers to those that increase the risk for the disease pathology. These include, but are not limited to, known major genetic mutations for the disease (including Chromosome 21 ß-APP mutations, Chromosome 14 Presenilin 1 mutations, and Chromosome 1 Presenilin 2 mutations), the polymorphism for apolipoprotein E (APOE-ε4), other genes that contribute risk for AD; Down syndrome and head injury. The second type refers to risk factors for disease expression. These include factors that affect development, growth and shrinkage of the brain across the life course, as well as the development of cognitive strategies for optimum utilization of the brain in individuals who carry pathology for AD. Accumulating evidence shows that some of the factors that improve reserve also may have effects on neuropathology as well.
In Chapter 10, we will consider the genetic factors that have been shown to increase the risk of AD and consider how much of the illness is determined by genes. In Chapter 11, we will discuss known and possible links between perinatal and early-life family conditions, such as the intrauterine environment, birth weight, birth order and sibship size, and late-life cognition. Other conditions relevant to early life, including paternal social class, poverty and deprivation in childhood, have begun to be studied in a few cohorts with very long follow-up times. In discussing other influences on AD from early life, we will consider education, IQ, and linguistic ability as well.
The remaining chapters in Section 3 are devoted to adult life risk factors. We will consider head trauma, smoking and alcohol consumption, the role of vascular disease in AD, diet, physical and cognitive exercise, social engagement, and medications that might be inversely related to AD risk, focusing on nonsteroidal anti-inflammatory drugs, statins, hormone replacement therapy, and anticholinergic medications.
In the context of the threshold theory, we can view clinical expression factors that increase AD risk as hastening clinical onset to earlier ages given a fixed genetic risk, and those that decrease AD risk as delaying clinical onset to later ages given the same genetic risk. Brookmeyer, Gray, and Kawas (1998) calculated the potential effects on the prevalence of AD of interventions that would delay the age at which individuals clinically manifest symptoms. They report that an intervention (or set of interventions) that reduced the overall risk for AD by 25% would result in a mean delay of 2 years, while an intervention that reduced AD risk by 50% would result in a mean delay of 5 years. The latter intervention would decrease the prevalence of AD in the year 2027 by almost half (52.5%) (Brookmeyer et al., 1998). Clearly then, prevention across the lifespan is an avenue that should be pursued in addition to finding medications that can reduce the pathology of the disease.
History and Methodological Aspects of Analytic Studies of AD: Case–Control Studies
Case–control studies, by virtue of their generally lower costs and relatively fast completion, were conducted as the first step in the systematic investigation of the etiology of AD. This study design was most common in the 1970s and 1980s. There are surprisingly few reports in the literature summarizing the results and methodological shortcomings of these studies. The case–control study gave epidemiologists a jumping-off place, beginning with what is fondly and at the same time disparagingly termed “fishing expeditions.” Fishing expeditions are done when little is known about a field. Investigators examine a large number of exposures in one case–control study. These may include risk and protective factors that already have some support from earlier studies (e.g., age and family history of memory problems), seem biologically plausible (e.g., head trauma, smoking), or that give rise to other diseases (e.g., pesticides in Parkinson’s disease, diabetes for vascular disease). This in turn can produce spurious findings (Type I errors) if the number of comparisons is large and no correction for multiple comparisons is used. There was the danger in the case–control study era that a statistically significant finding may have been due to chance. One of many examples of this is the report from a case–control study that nose-picking was associated with later-onset AD (ORmatched = 7.0 [7/1 discordant pairs, p = 0.08]), and physical underactivity was associated with earlier-onset AD (ORmatched = not calculable due to a zero in the denominator [14/0discordant pairs, p = 0.0005]) (Henderson et al., 1992). At a meeting where these findings were presented, one of our colleagues joked to one of us, “To stop Alzheimer’s, we just have to stop sitting around and picking our noses.” Although this comment was obviously meant to be facetious, we must be cautious about interpreting results based on small numbers.
While the case–control studies likely produced some false-positive results, they may also have produced false-negative ones. In order to focus on the purest form of AD, most of these studies chose to exclude possible AD by NINCDS-ADRDA criteria, eliminating cases where the relatively common vascular lesions could be contributing to disease expression. By focusing on probable AD cases without evidence for stroke or cerebrovascular disease, individuals with vascular risk factors for these outcomes were excluded from the cases, but not from the controls. Consequently, risk factors such as hypertension, diabetes, and hypercholesterolemia were not identified as risk factors for AD in the case–control studies. When prospective cohort studies began, participants unselected for vascular risk factors at baseline were followed for development of incident AD, permitting the important role of vascular risk factors in the clinical expression of AD to be observed. In fact, prospective cohort studies sometimes obtained the opposite findings from case–control studies. For example, case–control studies suggested that cigarette smoking, a risk factor for stroke, might be inversely related to AD. Cohort studies gave us the opposite answer, that cigarette smoking was a risk factor (Chapter 13). Cohort studies have also permitted the examination of risk factors for other dementia subtypes, such as Lewy body dementia and frontal temporal dementia.
Most of the cases in case–control studies were identified from dementia clinics or through hospital records. A selection bias is likely present in cases who were brought to medical attention by their family members. If family members were in denial, the patients may not come to medical attention until a moderate-to-severe dementia is present. Other AD patients may not come to medical attention at all, because they lived alone and did not have close family members to observe their condition and bring them to medical attention. In addition, if a demented individual identified in a clinic had no identifiable proxy informant, they would usually have been excluded from case–control studies.
The use of proxy informants is necessary for dementia patients who cannot provide valid information about their own exposures. However, their use invites information bias. Case proxies may either overreport or underreport past exposures, depending on their own recall, level of background reading, and desire to pin the cause on an identifiable event, such as a head injury. Furthermore, recall bias can be aggravated by control proxies underreporting exposures. Proxies are frequently selected from the next-of-kin who brings the patient in. This will most often be a spouse or an adult child. For some types of remote information, such as information about early life and adolescence, siblings may be better informants. The proxy type was usually not matched in the cases and controls, which could result in odds ratios biased either toward or away from the null value of 1.0.
When proxy informants must be used for cases, they should also be used for controls (Nelson, Longstreth, Koepsell, & van Belle, 1990). In an attempt to evaluate the quality of the information obtained from proxy informants, some case–control studies of AD conducted a validation study of control and control–proxy informant pairs to measure the degree of agreement between the two sources of information. The assumption of such validation studies was that the agreement between case–case proxy informant pairs would be similar to control–control proxy informant pairs. This is not necessarily true. For example, in a case–control study matching on informant type (we only accepted spouse informants), we rated exposure to chemicals in the cases’ and controls’ occupations two ways by asking the spouse and by assessment by an industrial hygienist who was blinded to case–control status. Figure 9.1 shows the results for one chemical exposure (Graves, A. Borenstein, unpublished). Epidemiologists usually assume that case proxies over-recall exposures due to the natural instinct to identify a cause for the disease. In this study, the sensitivity of reporting positive exposure was higher (83%, compared to an objective and blinded assessment made by an industrial hygienist) among case spouses, than among control spouses (61.5%). The specificity of reporting exposures by spouses was the same for both cases and controls, implying that if the industrial hygienist rated the occupation as not exposed to a certain chemical, both case and control spouse proxies were equally likely to rate it as nonexposed. These findings suggest that control informants may be more likely to under-recall exposures than case informants to over-recall exposures.
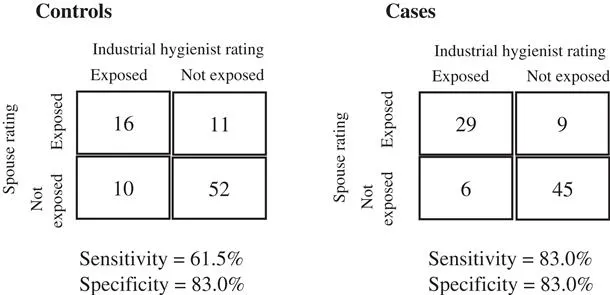
Table of contents
- Cover
- Front-matter
- Table of Contents
- Copyright
- Dedication
- Preface
- Acknowledgments
- Prologue: A Primer on Epidemiologic Concepts and Methods
- List of Illustrations
- List of Tables
- Chapter 1 : The “First” Case
- Chapter 2 : Clinical Appearance, Progression, and Classification
- Chapter 3 : Epidemiologic Definition of a Case
- Chapter 4 : Neuropathology of Alzheimer’s Disease
- Chapter 5 : The Threshold Model of Dementia
- Chapter 6 : The Prevalence of Alzheimer’s Disease
- Chapter 7 : The Incidence of Alzheimer’s Disease
- Chapter 8 : Survival and Mortality in Alzheimer’s Disease
- Chapter 9 : Introduction to the Analytic Epidemiology of Alzheimer’s Disease
- Chapter 10 : Family History, Genetics, and Down Syndrome
- Chapter 11 : Early-Life Factors
- Chapter 12 : Traumatic Brain Injury
- Chapter 13 : Cigarette Smoking and Alcohol Consumption
- Chapter 14 : Vascular Disease
- Chapter 15 : Diet
- Chapter 16 : Physical Activity
- Chapter 17 : Cognitive Activity
- Chapter 18 : Social Engagement
- Chapter 19 : Nonsteroidal Anti-Inflammatory Drugs, Hormone Replacement Therapy, and Anticholinergic Medications
- Chapter 20 : Prodromal Markers of Disease or Causal Risk Factors? Depression, Olfaction, and Subjective Memory Complaints
- Chapter 21 : Fluid, Imaging, and Cognitive Biomarkers
- Chapter 22 : Risk Assessment and Prevention of Alzheimer’s Disease
- Chapter 23 : Summary and Recommendations
- References
- Index
- A
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Alzheimer's Disease by Amy Borenstein,James Mortimer in PDF and/or ePUB format, as well as other popular books in Psychology & Cognitive Neuroscience & Neuropsychology. We have over 1.5 million books available in our catalogue for you to explore.