eBook - ePub
Vascular and Neurological Changes in Early Diabetes
Advances in Metabolic Disorders, Vol. 2
- 620 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Vascular and Neurological Changes in Early Diabetes
Advances in Metabolic Disorders, Vol. 2
About this book
Advances in Metabolic Disorders, Supplement 2: Vascular and Neurological Changes in Early Diabetes covers knowledge of the vascular and neurological changes in early diabetes. The book discusses the prevalence of macroangiopathy in asymptomatic diabetes, the prevalence of asymptomatic diabetes in human atherosclerosis, and the observations made in seeking evidence for macroangiopathy, microangiopathy, and neurological changes in patients with latent diabetes. The text also describes angiopathy and neuropathy in mild juvenile diabetes; the role of insulin in the development of atherosclerosis; and the effect of insulin on lipid metabolism of human arteries. Discussions about microangiopathy, including topics on serum glycoprotein disturbances and their rheological effects in diabetes mellitus; the biochemical properties of human glomerular basement membrane in normal and diabetic kidneys; and the plasma levels of growth hormone and glucagon in diabetic patients and relatives of diabetic patients are also considered. The book further tackles topics about neuropathy, including the role of sorbitol pathway in neuropathy, the polyol pathway in the neuropathy of early diabetes, as well as nervous abnormalities in early diabetes. The text concludes by looking into the effect of treatment on diabetes. Endocrinologist, biochemists, physiologists, and researchers working on related topics will find the book useful.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Internal Medicine & DiagnosisI
Macroangiopathy
Macroangiopathy — Its Prevalence in Asymptomatic Diabetes
H. Keen*† and R.J. Jarrett*, *Department of Medicine, Guy’s Hospital Medical School, London, England; †Invited speaker
Publisher Summary
This chapter describes the prevalence of macroangiopathy in asymptomatic diabetes. Disease of large and medium-sized arteries has come to be accepted as a major consequence of diabetes mellitus, occurring particularly in middle aged and older patients, and accounting for much of the morbidity and mortality of maturity-onset diabetics. The chapter describes a study in which a newly discovered diabetic group was characterized by 2 h blood sugars of 200 mg/100 ml or more. A normal control group was constituted of individuals with 2 h blood sugar levels below 120 mg/100 ml. Among men, there was no clear trend in the blood sugar category in individual age/sex groups. Among women, all certified cardiovascular deaths occurred either in diabetic or borderline subjects, but only in one age group did the numbers support the view that this was other than a chance association. In terms of cardiovascular mortality, there was no significant difference between the normal and the borderline subjects.
Disease of large and medium-sized arteries has come to be accepted as a major consequence of diabetes mellitus, occurring particularly in middle-aged and older patients and accounting for much of the morbidity and mortality of maturity-onset diabetics. This relationship does not go unchallenged, however, and it is disturbing that such astute observers as Mitchell and Schwartz (1965) and Pyke (1968) remain unconvinced of the reality of the association. Nor does the relationship occur universally. In Japan (Kuzuya and Kosaka, 1971; Goto and Fukuhara, 1968) and in other low atherosclerosis prevalence groups (Shaper et al., 1962), the incidence of coronary and peripheral arterial disease is also low among diabetics—little if at all higher than among corresponding nondiabetic population groups, and lower than among even the nondiabetic peoples of Europe and North America. Despite this clear-cut geographical difference in macrovascular disease, the frequency of microvascular disease is at least as high in Asian diabetic populations as in comparable Western groups.
Whatever its explanation, this dissociation of macro- and microvascular disease in Japanese and Western diabetics seriously weakens the argument that assigns an important role to the latter in the pathogenesis of the former. It also weakens the argument of those who ascribe impaired glucose tolerance to the effects of arterial disease, rather than vice versa. The dissociation supports the hope that atherosclerosis is not an inevitable consequence of diabetes in man, an observation that can be set alongside the assertion of Schettler (1970) of the absence of coronary disease in hypotensive diabetics. This apparent difference in atherosclerotic disease between East and West provides an important opportunity for carefully controlled transnational comparisons and a challenge, already perceived by Japanese colleagues, to try to examine the extent and the means by which Westernization of their way of life permeates the arterial wall as it penetrates the structure of the society.
In Europe, North America, and other Westernized populations, however, the increased prevalence of atherosclerosis in diabetics appears established beyond reasonable doubt. The relationship is most clear and can be partially quantified in epidemiologically based studies such as ours in Bedford, England (Keen et al., 1965), and those in Tecumseh, Michigan (Ostrander et al., 1965), Framingham, Massachusetts, (Kannel et al., 1967), Paris, France (Gelin et al., 1967), and Busselton, Australia (Welborn et al., 1968). These prevalence studies of atherosclerosis as it affects the coronary, limb, and cerebral circulation all point to an approximately 2 to 2l/2-fold excess involvement in the diabetic.
Prevalence studies tell only part of the story, however. They give a selective picture which emphasizes the lesser manifestations, underestimating those rendering the subject unavailable for study. A much clearer picture of the relationship is given by incidence studies which collect all the manifestations of disease over a period of time. There are very few published studies on the incidence of arterial disease in diabetic populations compared with suitable nondiabetic control groups. The main substance of this communication is to give the preliminary results of a 5-year incidence study in the three population groups defined in 1962 following the Bedford survey. The three glycemia groups were defined solely on the basis of their blood sugar levels measured 2 hours after 50 gm oral glucose on capillary blood using the AutoAnalyzer microferricyanide analytical method.
Methods and Materials
The three groups were defined as follows. A newly discovered diabetic group was characterized by 2-hour blood sugars of 200 mg/100 ml or more. A normal control group was constituted of individuals with 2-hour blood sugar levels below 120 mg/100 ml. It matched, by age and sex, an intermediate or “borderline diabetic” group with 2-hour blood sugars between 120 and 199 mg/100 ml. The newly found diabetics were referred to their family doctors after detection in 1962, and they determined further management with or without the help of the local diabetes clinic. These diabetics were re called for systematic review in 1967, and information on defaulters was sought out by a variety of means. The normal control subjects were similarly recalled approximately 12–15 months later and subjected to similar examination and also an investigation of defaulters.
The borderline group has been, and remains, under continuous scrutiny with regular visits to follow-up clinics every 6 months since 1962. For the purposes of this study, only the records of their visits in the first half of 1967 were referred to in order to make the degree of ascertainment comparable to that in the other two groups. Comparisons were based upon the application of standard WHO questionnaires regarding cardiovascular events (Rose and Blackburn, 1968)—angina pectoris, myocardial infarction, and intermittent claudication—to members of all three glycemia groups, and upon the certified cause of death of those who died during the 5-year follow-up period. Mortality ascertainment for the three groups was a little short of 100%. For morbidity information, however, it was 95% for the borderline group, 88% for the diabetics, and 82% for the normal controls.
Results
Figure 1 summarizes the 1962 prevalence estimates of arterial disease in the three glycemia groups, aggregated after suitable corrections for differences in age and sex composition. A similarly age/sex-adjusted aggregate of clinical arterial incidents, lethal and nonlethal, occurring during the follow-up period is shown in Fig. 2. This latter comparison is composed of questionnaire positive manifestations of morbidity and of deaths certified as cardiovascular in cause over the follow-up period, but does not include ECG changes. The gradient of arterial incidents with blood sugar is highly significant statistically (p < 0.01) and is steeper than the slope for prevalence. When the incidence aggregates are broken down into the component elements of morbidity and mortality by age and sex, however, the trend becomes less striking, although other features emerge.
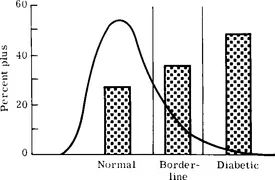
FIG. 1 Percentage frequency of “arterial disease” prevalence in rep...
Table of contents
- Cover image
- Title page
- Table of Contents
- ADVANCES IN METABOLIC DISORDERS
- Copyright
- List of Contributors
- Preface
- Acknowledgments
- Part I: Macroangiopathy
- Part II: Microangiopathy
- Part III: Neuropathy
- Part IV: Effect of Treatment
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Vascular and Neurological Changes in Early Diabetes by Rafael A. Camerini-Dávalos,Harold S. Cole in PDF and/or ePUB format, as well as other popular books in Medicine & Internal Medicine & Diagnosis. We have over 1.5 million books available in our catalogue for you to explore.