Classification
PEM is a term coined originally as ‘protein-calorie malnutrition’ to cover a spectrum of conditions ranging from marasmus at one extreme to kwashiorkor at the other. The term ‘marasmus’ is derived from the Greek marasmos meaning wasting and has been recognized for centuries as being, with gastroenteritis, a major cause of infant mortality. The term ‘kwashiorkor’ was first used by Dr Cicely Williams in 1933 to describe a condition that she recognized in the then Gold Coast. The word is taken from the Ga language of Ghana and literally means ‘the disease the first child gets when the second is on the way’.
In marasmus the child is underweight with very little body fat and consequent loosening of the skin. There is also muscle atrophy and, depending on the chronicity of the condition, short stature. Kwashiorkor, on the other hand, is characterized by skin and hair changes, oedema, ‘moon face’, fatty liver, hypoalbuminaemia and psychomotor changes. The clinical manifestations of this disease differ in different parts of the world, as also does the age of development. These differences have tended to lead to some confusion in nomenclature and classification of the different forms of PEM.
A classification of PEM should be suitable for use in:
1. The international classification of diseases
2. Prevalence studies and other observations in communities
3. Clinical and research investigations.
The simplest classification is that known as the Wellcome classification (Table 1.1), which is based simply on the deficit in body weight and the presence of oedema. This classification has advantages because of its simplicity, but it cannot be applied when the age of the patient is not known and does not take into account the chronicity of the disease process.
TABLE 1.1
WELLCOME CLASSIFICATION OF INFANTILE MALNUTRITION 2
| | Percentage of expected weight for age * | Oedema |
| Marasmus | < 60 | Absent |
| Marasmic kwashiorkor | < 60 | Present |
| Kwashiorkor | 60–80 | Present |
| Underweight | 60–80 | Absent |
*Taken as the 50th percentile of the Boston standards.3
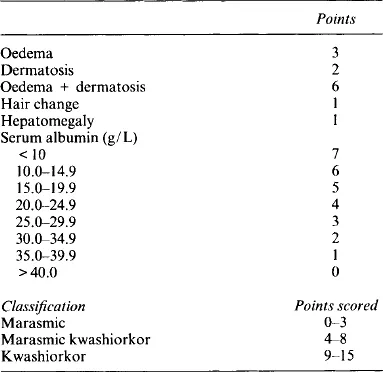
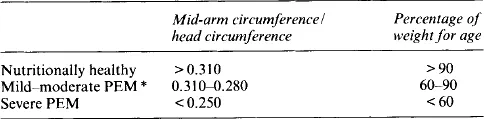
McLaren et al.4 introduced a simple scoring system for classifying the severe forms only (Table 1.2). This method is precise and provides a means of objectively classifying the type of patients likely to be hospitalized. It does, however, require access to laboratory facilities. Another method, introduced by Kanawati and McLaren5, requires only the use of a stiff tape-measure and is based on the ratio of mid-arm circumference to head circumference, which is independent of age at least from 3 months to 48 months and is similar for the two sexes (Table 1.3). This method is, however, rough, unsuitable for use in individual children and is intended for use only in screening large numbers.
TABLE 1.2
SIMPLE SCORING SYSTEM FOR PROTEIN–ENERGY MALNUTRITION4
TABLE 1.3
ASSESSMENT OF MARGINAL MALNUTRITION 5
*PEM, protein-energy malnutrition.
It seems desirable that any classification of PEM should take into account deficits in weight and height for age. One such classification is shown in Table 1.4. The diagnosis of the kind of severe PEM with which the child presents, kwashiorkor or marasmus, may change quickly for if oedema is lost a kwashiorkor child becomes a marasmic one.
TABLE 1.4
CLASSIFICATION OF NUTRITIONAL STATUS IN EARLY CHILDHOOD6†
| Classification | Observed weight as percentage of ideal weight/length age |
| Overweight | > 110 |
| Normal range | 90–109 |
| Mild PEM* | 85–89 |
| Moderate PEM | 75–84 |
| Severe PEM ** | < 75 |
*PEM, protein-energy malnutrition.
**Marasmus (no oedema) or kwashiorkor (with oedema).
†Authors give a nomogram for rapid calculation and classification.
Pathogenesis
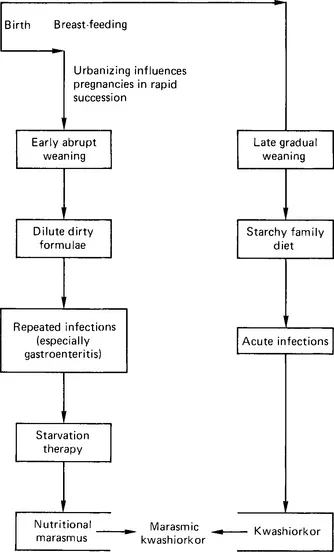
Although PEM is a nutritional deficiency disease, it is doubtful if nutrition can ever be separated from the whole variety of social factors that makes up the complex environment in which children grow up. Thus, economic stringencies, overcrowding, poor hygiene, and religious and other taboos all contribute to the development of the condition. The exact form of PEM that develops depends on the age of the child, the duration of breast-feeding and also on weaning practices. Industrialization has influenced the nature of the most prevalent types of PEM in different communities. From an analysis of these factors. in the Lebanon and in Jordan, McLaren7 put forward a scheme (Fig. 1.1) to account for the pathogenesis of the extreme forms.
Figure 1.1 Paths leading from early weaning to nutritional marasmus and from protracted breast feeding to kwashiorkor.
Classically it was held that marasmus is caused by a shortage of food, predominantly of energy, and that kwashiorkor is caused by a shortage of protein of the right kind but that the energy supply might be adequate. It has become clear that this simplistic view is a misconception, and that this has had important consequences for it has led to the idea that there is a ‘protein gap’, which has been described, in fact, as a ‘protein fiasco’. In India, children have been described as developing either marasmus or kwas...