- 1,008 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Peripheral Nerve Disorders
About this book
Disorders of the peripheral nervous system (PNS) are the cause of prominent neurological symptoms including weakness, sensory loss, pain and autonomic dysfunction associated with deficits, morbidity and mortality. These disorders may be primary hereditary or cryptogenic neurologic disorders confined to the PNS or part of the pathology of both the central nervous system and the PNS. Most PNS disorders are secondary to other system disorders and may be responsive to treatment of the primary disease. Important advances have been obtained in several areas including molecular genetics, biochemistry, immunology, morphology and physiology that have enhanced our understanding of the causes and consequences of damage to peripheral nerve. Understanding of both these groups of PNS diseases has greatly expanded over recent years and has led to important advances of treatment both to protect and to repair damages of peripheral nerve. This volume provides an overview of the state-of-the-art of examination, diagnosis and treatment of these very diverse disorders and will be of interest to both the research and clinical neuroscience and neurology communities.
- Covers both hereditary and cryptogenic neurologic disorders
- Includes advances in the basic science of PNS from molecular genetics, biochemistry, immunology, morphology and physiology
- Detailed coverage of neuropathy in connective tissue disorders, infectious disorders, metabolic disorders and malignancy
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
Section 1: Introduction
Outline
Chapter 1 Prelude to the peripheral neuropathies
Chapter 1
Prelude to the peripheral neuropathies
Arthur K. Asbury1 and Michael J. Aminoff2, 1Department of Neurology, Hospital of the University of Pennsylvania, Philadelphia, PA, USA, 2Department of Neurology, School of Medicine, University of California, San Francisco, CA, USA
Recognition of, and interest in, peripheral neuropathies began to evolve almost two centuries ago, mainly in the UK and the rest of Europe, and then in the USA. The newly developing techniques of histopathology during the 19th century made it possible to study peripheral nerves and nerve roots at autopsy and in experimental studies in animals. Clinicopathological studies, notably by Jean-Martin Charcot and his students in Paris but also by others, allowed correlation with the clinical findings recorded during life. Even persons who had recovered from a nerve root or nerve trunk neuropathy with minimal or no persisting symptoms or findings, and who then lived for many years, were often found at autopsy to have residual pathological findings in the previously affected neural structures. The clinicopathological approach of correlating the clinical features with the postmortem neuropathological findings has now been in place for over 150 years. It has formed the base of much of the knowledge of peripheral neuropathy, but it has not indicated how to diagnose, manage, and ultimately reverse all such disorders.
The remarkably insightful clinical studies by Silas Weir Mitchell and his colleagues on casualties of the American Civil War in the latter half of the 19th century also led to further interest in the peripheral nervous system, at least for a time. Mitchell’s work with George Morehouse and William Keen was summarized in their pioneering book Gunshot Wounds, and Other Injuries of Nerves (1864), which contained the first descriptions of causalgia. Mitchell subsequently extended this into his definitive Injuries of Nerves and Their Consequences (1872), the first substantive work detailing the symptoms, signs, treatment, and outcome of nerve injuries.
Despite these advances on both sides of the Atlantic, there was little interest in the peripheral nervous system for many years. Indeed, until the 1950s, peripheral neuropathies were of relatively minor interest to most neurologists, who were occupied principally with the many disorders affecting the central nervous system. As such, peripheral nerve disorders were not given the attention they deserved, and patients with these disorders were often managed by other physicians, particularly internists and general physicians.
This situation in 1950 was particularly evident in the USA. There, physicians who wished to specialize in the disorders of the nervous system generally received 2 years of training, 1 year of neurology and 1 year of psychiatry, and often became skilled in neither. Those specialists of yesteryear were little interested in, and poorly knowledgeable of, disorders of the peripheral nervous system. Since that time, however − with the advent of precise, objective methods of studying peripheral nerve function − these disorders have assumed greater importance.
In the 19th and 20th centuries, basic and clinical neurophysiologists began to develop techniques that allowed for a greater understanding of peripheral nerve function and led to quantitative methods for evaluating neuromuscular function in health and disease. Guillaume Duchenne de Boulogne in Paris, Emil Heinrich du Bois-Reymond in Berlin, and Wilhelm Erb of Heidelberg were early (19th century) pioneers in the field of electrodiagnosis or electrophysiology, followed later by Charles Sherrington and Edgar Adrian in Britain and by Joseph Erlanger, Herbert Gasser, and George Bishop in the USA, who worked on the selective functions of single nerve fibers and related issues. The mechanism of nerve conduction and the events at the neuromuscular junction only became clearer in the latter half of the 20th century, however, with the fundamental studies of J. Z. Young, Alan Hodgkin, Andrew Huxley, Bernard Katz, Ricardo Miledi, and many other physiologists and scientists. Adrian and Bronk recorded the electrical activity of motor units with a concentric needle electrode in 1929, allowing the recruitment pattern of motor units and regulation of muscle force to be studied. Within 10 years, Derek Denny-Brown had described the electrophysiological hallmark of fibrillation and fasciculation potentials in muscle, and shortly thereafter Fritz Buchthal in Copenhagen began describing the electrophysiological features of a number of neuromuscular diseases, often in a quantitative manner. Erik Kugelberg in Stockholm, Roger Gilliatt and P.K. Thomas in London, and Edward Lambert in Rochester, Minnesota, were other pioneers in clinical neurophysiology, and their work led to the widespread clinical application of objective techniques for measuring peripheral nerve function and permitted the characterization and localization of disordered function, even when the disorder had not yet become manifest clinically.
Detailed pathological, ultrastructural, microbiological, immunological, and genetic studies soon followed. These were important, but as many of the leaders in these fields are still living − and indeed have contributed to these volumes − they will not be named individually here. The reader will be able to recognize their contributions in the chapters that follow. Through the application of these various techniques, many new disorders have come to be recognized, as is discussed in later chapters. These developments aroused the interests of young trainees in neurology, and the subspecialty of neuromuscular diseases is now one of the most popular areas in neurology, with neuromuscular specialists making up something more than 15% of all fully-trained neurologists.
The body of knowledge concerning neuromuscular medicine in general and peripheral neuropathies in particular has grown exceptionally rapidly over the past five or six decades, as can be seen from the breadth of this book, and this already large body of knowledge will surely continue to grow. More than 50 chapters following this one set forth in great detail the most modern ways of evaluating, characterizing, distinguishing, and managing the numerous specific neuropathic syndromes that have been described. Some disorders are related to systemic disorders such as porphyria, uremia, sarcoidosis, systemic amyloidosis, diabetes mellitus, or vasculitis. Others are due to exogenous toxins such as alcohol or other drugs such as long-term anti-epileptic medication. The list of possible causes underlying a given polyneuropathy is large. It is easy for physicians to overlook the responsible culprit in individual cases. Many neuropathies are amenable to treatment or avoidance of the responsible cause. Virtually all of the irreversible neuropathies can be managed by specialists to lessen the symptoms and minimize the difficulties of everyday life.
The editors of this two-volume work have taken on an enormous task in organizing and summarizing present-day knowledge of the peripheral nervous system and the myriad disorders that affect it. Their work will benefit not only the medical and scientific community, for whom these volumes will serve as a useful reference, but also members of the general public who will benefit by the application of this knowledge in an individual setting. They are to be congratulated on their achievement.
Section 2: Structure and function
Outline
Chapter 2 Microscopic anatomy
Chapter 3 Gross anatomy and development of the peripheral nervous system
Chapter 4 Physiology and pathophysiology of myelinated nerve fibers
Chapter 5 Biology of Schwann cells
Chapter 6 Neurophysiological approach to disorders of peripheral nerve
Chapter 7 Testing the autonomic nervous system
Chapter 8 Imaging of the peripheral nervous system
Chapter 9 The nerve biopsy
Chapter 10 The cutaneous nerve biopsy
Chapter 11 Antibody testing in peripheral nerve disorders
Chapter 12 DNA testing in hereditary neuropathies
Chapter 2
Microscopic anatomy
normal structure
Rosalind King*, Department of Clinical Neurosciences, Institute of Neurology, University College London, Royal Free Campus, London, UK,*Correspondence to: Rosalind King, Ph.D., Department of Clinical Neurosciences, Institute of Neurology, University College London, Royal Free Campus, Rowland Hill St., London NW3 2PF. Tel: + 44 (0)207 472 6364, Fax: + 44 (0)207 472 6829, Mobile: + 44(0)7725489013, E-mail: [email protected]
Abstract
A peripheral nerve trunk is composed of nerve fascicles supported in a fibrous collagenous sheath and defined by concentric layers of cells (the perineurium) that separate the contents (the endoneurium) from its fibrous collagen support (the epineurium). In the endoneurium are myelinated and unmyelinated fibers that are axons combined with their supporting Schwann cells to provide physical and electrical connections with end-organs such as muscle fibers and sensory endings. Axons are tubular neuronal extensions with a cytoskeleton of neurotubules and tubulin along which organelles and proteins can travel between the neuronal cell body and the axon terminal.
During development some axons enlarge and are covered by a chain of Schwann cells each associated with just one axon. As the axons grow in diameter, the Schwann cells wrap round them to produce a myelin sheath. This consists of many layers of compacted Schwann cell membrane plus some additional proteins. Adjacent myelin segments connect at highly specialized structures, the nodes of Ranvier. Myelin insulates the axon so that the nerve impulse can jump from one node to the next.
The region adjacent to the node, the paranodal segment, is the site of myelin terminations on the axolemma. There are connections here between the Schwann cell and the axon via a complex chain of proteins. The Schwann cell cytoplasm in the adjacent segment, the juxtaparanode, contains most of the Schwann cell mitochondria.
In addition to the node, continuity of myelin lamellae is broken at intervals along the internode by helical regions of decompaction known as Schmidt−Lanterman incisures; these are seen as paler conical segments in suitably stained microscopical preparations and provide a pathway between the adaxonal and abaxonal cytoplasm.
Smaller axons without a myelin sheath conduct very much more slowly and have a more complex relationship with their supporting Schwann cells that has important implications for repair.
Key words
nerve fascicle; nerve fibers; artefacts; myelin; Schwann cells; axons; nerve conduction; electron microscopy; development
The nerve trunk
Microscopic study of nerve structure goes back at least to 1837 with the studies of Remak (Remak, 1837, 1838) followed a year or two later by those of Schwann (Schwann, 1839). Both these names are preserved in modern nomenclature; Schwann cells are the support cells for axons and Remak fibers is a convenient shorthand term for unmyelinated axons and their associated Schwann cells. Even earlier, in 1781, Fontana described the curious patterning seen by oblique illumination on the surface of fresh nerve trunks that is now known as the spiral bands of Fontana (Fontana, 1781). This has a regular wavy appearance that may be altered by stretching the fascicle or peeling off the perineurium. Much more recently, the relationship of this pattern to the layers of collagen in the fascicle has been studied in detail and shown to be in register around the entire surface of the nerves and also within the fascicle. Collagen fibrils are inextensible so the function of this arrangement is probably to allow stretching and deformation of the nerve trunk without damage to the nerve fibers (Stolinski, 1995).
The nerve trunk is composed of several fascicles, each of which is defined by cylindrical layers of flattened squamous cells forming the perineurium, and embedded in a collagenous matrix, the epineurium (Fig. 2.1). Nerve fibers consisting of axons and their associated Schwann cells and, in some cases, a myelin sheath, lie together in these fascicles and are given mechanical support by endoneurial fibrous collagen and metabolic support from a network of small blood vessels. These axons are extensions of neuronal cell bodies located in the central nervous system or the dorsal root ganglia. They leave the neuronal perikaryon at the axon hillock and are unbranching along the greater part of their length until they reach their terminus where they divide into many small fibers.
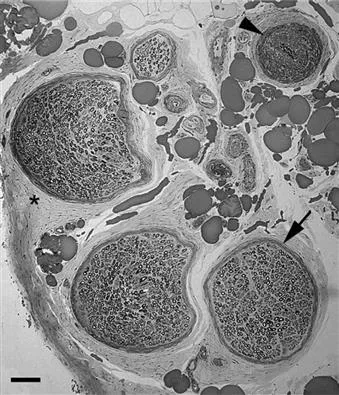
Fig. 2.1 Low power micrograph of three large and one small fascicle defined by perineurium (arrow) and embedded in epineurial collagen (*) and fat. There are several small blood vessels and a larger arteriole (arrowhead). Scale bar = 50 μm.
Nerve fibers
Myelinated fibers
All axons are associated with, and dependent on, Schwann cells. In the case of larger diameter fibers (dia...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Handbook of Clinical Neurology 3rd Series
- Foreword
- Preface
- Contributors
- Section 1: Introduction
- Section 2: Structure and function
- Section 3: Clinical aspects
- Section 4: Plexus and compression lesions
- Section 5: Inflammatory root and nerve lesions
- Section 6: Neuropathy in connective tissue disorders
- Section 7: Neuropathy in infectious disorders
- Section 8: Neuropathy and metabolic disorders
- Section 9: Neuropathy and malignancy
- Section 10: Cryptogenic, traumatic and iatrogenic neuropathies
- Section 11: Familial neuropathies
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Peripheral Nerve Disorders by Gérard Said,Christian Krarup in PDF and/or ePUB format, as well as other popular books in Medicine & Neurology. We have over one million books available in our catalogue for you to explore.