eBook - ePub
Fetal Physiology and Medicine
The Basis of Perinatology
- 838 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Fetal Physiology and Medicine
The Basis of Perinatology
About this book
Fetal Physiology and Medicine: The Basis of Perinatology, Second, Revised Edition documents many of the major advances in fetal medicine, including developmental physiology, pathology, and therapy. This book covers the most important areas of maternofetal medicine and presents different views of the critical problems of development. The various components of fetal metabolism are highlighted to demonstrate how animal experimentation has given a clear view of the interrelationship of the mother, placenta, and fetus. This text is comprised of 24 chapters; the first of which describes the use of ultrasound in antenatal diagnosis of congenital structural anomalies. This topic is followed by a discussion on sexual differentiation, acquired immunity, and endocrine changes, as well as the physiology of breathing, the control of the fetal cardiovascular system, lung maturation, fetal infections, and the effects of hypoxia on the fetal brain. This book also provides comprehensive reviews of fetal regulatory mechanisms, such as the reninangiotensin system, water metabolism, and fetal and placental hormone production. Other chapters focus on clinical applications, such as antenatal fetal heart rate monitoring, the technical aspects of fetal and uterine pressure measurements, fetal acid-base balance, and the prevention of preterm delivery. A section that explores the transition from intrauterine to extrauterine life concludes this book. This source is of great potential value to all students and practitioners of reproductive medicine.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Antenatal Diagnosis of Congenital Structural Anomalies with Ultrasound
Greggory R. DeVore*, Yale University School of Medicine, New Haven, Connecticut
John C. Hobbins, Yale University School of Medicine, New Haven, Connecticut
Publisher Summary
This chapter discusses antenatal diagnosis of congenital structural anomalies (CSAs) with ultrasound. CSAs encompass a broad spectrum of conditions, including those with minimal involvement and disability and those incompatible with extrauterine life. With the advent of ultrasound, CSAs that grossly alter normal fetal anatomy can be screened for and detected as early as the second trimester of pregnancy. The fetus is ideal for ultrasound evaluation because it is floating in a fluid medium that provides maximum contrast with fetal tissues and, thus, optimum fetal anatomical characterization. With the advent of diagnostic ultrasound, many pregnancies at risk for congenital structural anomalies can be accurately evaluated and the anomaly either diagnosed or excluded. If excluded, the pregnancy can continue with the assurance that the chance of giving birth to an affected fetus is quite low. Those congenital anomalies amenable to surgical repair following birth have also been diagnosed with ultrasound. This allows for optimal care of the newborn at a center equipped with a newborn intensive care unit as well as pediatric surgeons.
INTRODUCTION
Congenital structural anomalies (CSAs) encompass a broad spectrum of conditions, those with minimal involvement and disability (polydactyly) to those incompatible with extrauterine life (anencephaly, renal agenesis, etc.). The etiology of CSA may be grouped into four classes: unknown (65-70%), environmental factors (10%), genetically transmitted diseases (20%), and chromosomal aberrations (3-5%) (Wilson, 1973).
Until recently the prenatal diagnosis of CSA was limited to those which could be detected during the second trimester by either biochemical or chromosomal aberrations noted in analysis of amniotic fluid obtained following amniocentesis (Sandstrom and Milunsky, 1977). With the advent of ultrasound, CSAs which grossly alter normal fetal anatomy can be screened for and detected as early as the second trimester of pregnancy (Table. 1).
Table 1
Diagnosis of Congenital Anomalies Made in the Second Trimester in Patients Genetically at Risk for Fetal Deformity (1976-1980)a
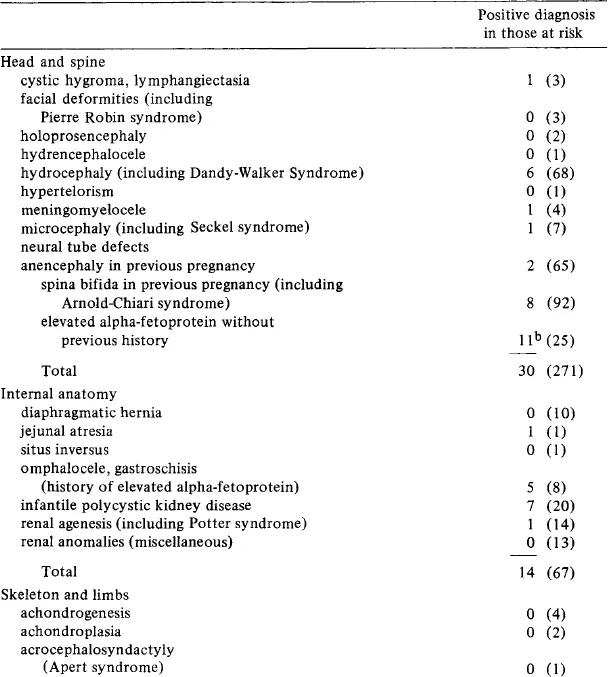
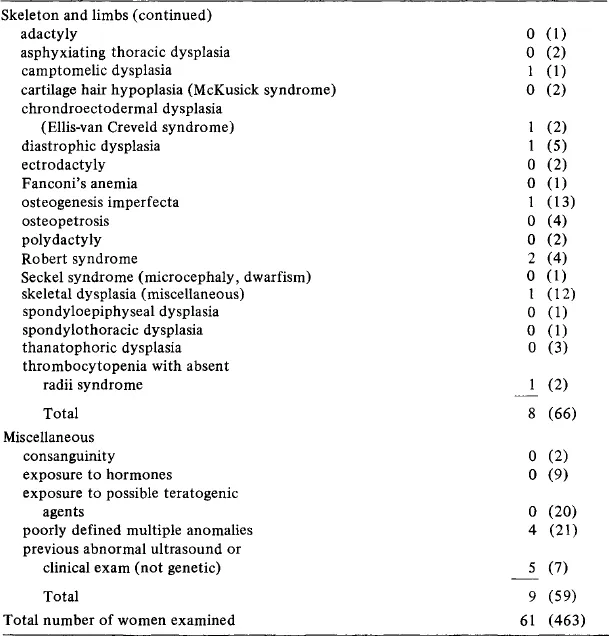
aFiguies in brackets show the number of women examined.
bIncludes spina bifida (5), omphalocele (3), meningomyelocele (1), jejunal atresia (1), and hydrocephaly (1).
ULTRASOUND
The fetus is ideal for ultrasound evaluation because it is floating in a fluid medium which provides maximum contrast with fetal tissues and, thus, optimum fetal anatomical characterization.
Initially, ultrasound consisted of a bistable white on black image which only allowed for the evaluation of gross fetal structures (Figure. 1A). As the electronics became more sophisticated, the bistable image changed to one with 16 shades of gray. Structures not seen with the bistable image were observed with gray-scale ultrasound, thus allowing for a more detailed visualization of fetal anatomy (Figure. 1B).
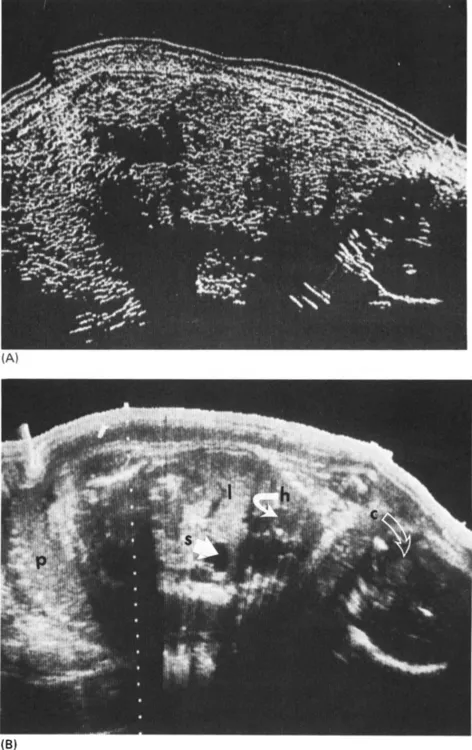
Figure 1 Identical sagittal scans of a 26-week fetus using (A) bistable and (B) gray-scale formats (s, stomach; h, heart; c, cranium; 1, liver; p, placenta).
Although gray-scale ultrasound greatly improved imaging, one of the limitations was that the image was always static; that is, it did not allow for analysis of the active, moving fetus. Real-time ultrasound, which incorporates gray scale, added another dimension to ultrasound, since the still image suddenly became “alive.” This made it possible to evaluate the fetus as it moved about in its intrauterine environment and to observe pulsating vascular structures such as the fetal heart, aorta, and intracranial arteries.
To accurately evaluate the fetus for CSA therefore requires (1) a static contact gray scale as well as a real-time scanner, (2) a thorough knowledge of normal fetal anatomy as depicted by ultrasound, and (3) a complete understanding of the defect expected to be seen when evaluating a fetus for a specific anomaly.
The following review will focus on the use of diagnostic ultrasound in the diagnosis of the more commonly seen structural anomalies which have been studied in either the second or third trimester of pregnancy.
DIAGNOSIS OF CONGENITAL STRUCTURAL ANOMALIES IN PREGNANCIES NOT KNOWN TO BE AT RISK
Unfortunately, CSAs are most often diagnosed at birth or shortly thereafter. This can present many problems for both the family and the physician. It is not unheard of for an obstetrician to perform a cesarean section for fetal distress occurring during labor only to find a grossly malformed fetus which dies shortly after birth.
Although some physicians advocate an ultrasonic scan for all pregnant women, this is not widely practiced worldwide. When an ultrasound scan is requested, the report usually contains information concerning the biparietal diameter, with the corresponding gestational age, the location of the placenta, the number of fetuses, and the lie of the fetus, and it may or may not indicate the relative quantity of amniotic fluid present.
Although not specific, the quantity of amniotic flui...
Table of contents
- Cover image
- Title page
- Table of Contents
- REPRODUCTIVE MEDICINE
- Copyright
- Foreword
- Preface
- Contributors
- Chapter 1: Antenatal Diagnosis of Congenital Structural Anomalies with Ultrasound
- Chapter 2: Sexual Differentiation
- Chapter 3: Ontogeny of Acquired Immunity and Maternofetal Immunological Interactions
- Chapter 4: Endocrine Pancreas of the Pregnant Mother, Fetus, and Newborn
- Chapter 5: Fetal Fat and Glucose Metabolism
- Chapter 6: Maternal, Fetal, and Neonatal Amino Acid and Protein Metabolism
- Chapter 7: Diabetes Mellitus and the Fetus
- Chapter 8: Fetal Breathing
- Chapter 9: Physiological Control of the Fetal Cardiovascular System
- Chapter 10: Fetal Lung Maturation and the Respiratory Distress Syndrome
- Chapter 11: Maternal and Fetal Infection
- Chapter 12: Factors Influencing Perinatal Wastage
- Chapter 13: Effect of Hypoxia on Fetal Brain
- Chapter 14: Renin-Angiotensin System in Early Life
- Chapter 15: Mineral and Water Exchange between Mother and Fetus
- Chapter 16: Regulation of Fetal Growth
- Chapter 17: Fetal, Placental, and Maternal Hormones
- Chapter 18: Energy and Substrate Requirements for Fetal and Placental Growth and Metabolism
- Chapter 19: Regulation of Myometrial Function throughout Gestation and Labor: Effect on Fetal Development
- Chapter 20: Antepartum Monitoring of Fetal Heart Rate
- Chapter 21: Technical Aspects of Fetal and Intrauterine Pressure Monitoring
- Chapter 22: Maternal and Fetal Acid – Base Balance and Blood Gas Measurement
- Chapter 23: Prevention of Preterm Delivery
- Chapter 24: Adaptation of the Newborn to Extrauterine Life
- Index
- About the Editors
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Fetal Physiology and Medicine by Richard W. Beard, Peter W. Nathanielsz, Richard W. Beard,Peter W. Nathanielsz in PDF and/or ePUB format, as well as other popular books in Medicine & Gynecology, Obstetrics & Midwifery. We have over 1.5 million books available in our catalogue for you to explore.