eBook - ePub
Healthcare Reform, Quality and Safety
Perspectives, Participants, Partnerships and Prospects in 30 Countries
- 384 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Healthcare Reform, Quality and Safety
Perspectives, Participants, Partnerships and Prospects in 30 Countries
About this book
This book offers a global perspective on healthcare reform and its relationship with efforts to improve quality and safety. It looks at the ways reforms have developed in 30 countries, and specifically the impact national reform initiatives have had on the quality and safety of care. It explores how reforms drive quality and safety improvement, and equally how they act to negate such goals. Every country included in this book is involved in a reform and improvement process, but each takes place in a particular social, cultural, economic and developmental context, leading to differing emphases and varied progress. Methods for tackling common problems - financing, efficiencies, effectiveness, evidence-based practice, institutional reforms, quality improvement, and patient safety initiatives - also differ. Representatives from each nation provide a chapter to convey their own situation. The editors draw a conclusion from these numerous contributions and synthesize the themes emerging into a coherent 'lessons learned' summary that delivers value to the numerous stakeholders. Healthcare Reform, Quality and Safety forms a compendium of the current 'state of the art' in global healthcare reform. This is the first book of its type, and offers a unique opportunity for cross-fertilization of ideas to the mutual benefit of countries involved in the project. The content will be of interest to governments, policymakers, managers and leaders, clinicians, teaching academics, researchers and students.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter 1
Introduction
The Genesis of This Compendium
As academic researchers, we have collectively and individually been interested in health reform for many years. Health reform at its most basic involves making changes (which are hoped to result in improvements) in the performance, operations, structures, process, or outcomes of health systems. (Of course, a key part of reform is to decide what to keep and what to change. Some things may be working well and not need reforming.) Nevertheless, reform is usually construed as a set of high-level, macro-system considerations concentrating on change. We have also been interested over the years in efforts to enhance the quality of care and make things safer for patients. Healthcare quality is a multi-faceted concept which embraces a number of dimensions, including: safety, cost-effectiveness, access, responsiveness, patient centeredness, and equity. Patient safety is about the prevention of harm to patients. Quality and safety interventions are typically thought of as targeted initiatives at the mid- to lower-levels of health systems—a set of meso- or micro-system considerations.
However, as we each conducted and participated in research on our own health systems, we rarely saw health reform explicitly related to quality and safety. It wasn’t clear to us how big-picture, national-level reforms stood in relation to measures to improve the quality of care and safety of patients.
So, guided by an initial idea from the first-listed editor to develop our understanding of these interactions, the editors met at various times over several years, in Sydney, Australia; Tokyo, Japan; Birmingham, England; and Hong Kong, People’s Republic of China, to consider a key question: what is the relationship between large-scale health system reforms and quality of care and patient safety? We did not expect that there would be a simple answer. We doubted that health reform and quality and safety would have a definite, positive relationship, because we know that healthcare is delivered in a complex adaptive system, and that complex constructs are rarely associated in a linear relationship. We also hypothesized—speculated, really—that disentangling the effects of health systems reform at the national level on quality and safety delivered at the front lines of care, would not be easy. However, it is a sufficiently important topic—if only because, at least in principle, the two should be related in a coherent, well-functioning system. We agreed to allocate some serious intellectual resources to analyzing it.
The Involvement of 30 Health Systems
To give effect to our interest in how, or whether, health reforms affect the quality and safety of care delivered on-the-ground in health systems, we set off in search of a way to inquire into the phenomenon. The first-listed editor hit on the idea of a book of invited chapters from a variety of health systems on the topic, and persuaded the other editors to join in support. We invited representatives from multiple countries, and ended up with over 30 countries each to give a talk at the International Society for Quality in Health Care (ISQuA) annual meeting held in Edinburgh, Scotland, in October 2013. Each country made a presentation and most accepted our subsequent invitation to develop a chapter for the book. Over the next six months, each devoted some of their valuable time to explicating their answer to the question we had posed.
We recognized a unique and very special opportunity. By inviting a range of lower-, middle-, and higher-income countries to contribute a chapter, we were poised to address, head-on, a problem that most international books on health systems fail to solve: to ensure there is adequate representation of countries beyond those in the Organization for Economic Cooperation and Development (OECD). In this, the final version of the book, as can be seen, we were successful in this quest, and we have assembled chapters from each of the key regions of the world.
The book provides an in-depth analysis of 24 health systems, in addition to a regional perspective provided on the Gulf States written by colleagues in the Kingdom of Saudi Arabia, adding a further six countries. In total, 30 health systems, providing care to more than four billion people, over 60 percent of the world’s population, living in over 51,762,891 square kilometers of the earth, are represented (Figure 1.1) (worldatlas n.d.).
What Do We Know About This Issue to Date?
There are various sources of information which enable policymakers, researchers, and other interested parties to appreciate how healthcare systems are structured or perform comparatively. These include data sources and studies from the Commonwealth Fund in the United States, academic studies published in journals such as Health Policy, Health Policy and Planning, BMJ Quality & Safety, and International Journal for Quality in Health Care, and from reports and health systems or country profiles from the OECD, World Health Organization (WHO), the United Nations (UN), and the International Labour Organization (ILO).
From these sources, a set of meta-level conclusions can be drawn. At their most basic, health systems consume a sizeable proportion of their countries’ gross domestic product (GDP), and each face logistical challenges in delivering care equitably and efficiently across the populations they serve. Although healthcare must be targeted to localized and specific groups, equally it is always a national concern, too. Further, regardless of country, delivering healthcare to citizens is never merely an economic, financial, social, or logistical problem. It is also, inevitably, intensely political and ideological.

Figure 1.1 Representation of countries within the book
All health systems are accountable for spending budgetary allocations wisely and organizing care to meet needs. They are structured across sectors—acute, primary, secondary, tertiary, aged care, and community-based services. Every health system has a mix of publicly-funded and privately-provided services, although the particular balance of service provision across the public and private spheres differs greatly by country.
A key concern of health systems is to get the policy and legislative settings right, and there are always multiple measures in train in every country to improve, tweak or revamp the system. This is health reform—adjusting policy, legislative requirements, structures, responsibilities, funding mechanisms, and the like. There are also strenuous efforts, often funded as projects, programs, and initiatives, to improve things at the organizational level. These take the form of measures such as mandating hand hygiene behaviors, introducing root cause analysis training, specifying the use of checklists in theatres, training staff to be better at detecting deteriorating patients, and standardizing approaches to shift handovers. Additional efforts are in play at the clinical coalface—where individual providers and care-giving teams work to make sense of national mandates and organizational policies, while trying to provide the best possible care to their patients.
How the Chapters and Book are Structured
We gave the leading authors of each chapter a template to serve as a guide, specifying key issues and more detailed points we hoped they would address. Many of the invited authors involved co-authors in their countries, and occasionally beyond, to work with them and provide additional input into their chapter. Most but not all chapter-writers found this template useful, with some preferring to write under their own, purpose-designed headings and subheadings. This was fine with us, as we did not want to be excessively prescriptive, preferring instead to see authors express their answer to the question we had set them in their own way. However, as you read each contribution, you will find that even when the headings differ from chapter to chapter, similar points seem to be touched on, recurrently, throughout the book.
We partitioned the book into five sections. These map to five key geographical regions. This may seem in hindsight a natural, even inevitable division, but the book could have been structured differently. We discussed this as we edited the chapters, thinking about whether readers might prefer to see chapters grouped alphabetically, or by income (with sections on lower-, medium-, and higher-income countries), or similarly financed (more privately-oriented systems like America’s and Japan’s clustered together, contrasted with more predominantly tax payer-funded systems, like those of Europe). But in the end, any grouping system seemed to rely on a superficial judgment and, in any case, a regional geographical structure worked best. Accordingly, we have sections of the book covering countries in Africa and Western Asia (Part I), Eastern Asia and Southern Asia (Part II), South Eastern Asia and Oceania (Part III), The Americas (Part IV), and Europe (Part V). Although we all did a share of editing chapters across different regions, we each took primary responsibility for editing an allocation: Parts I and III (JB), Part II (YM), Part IV (JJ), and Part V (RM).
Identifying Our Readers and the Place of the Book in Context
This book is written for healthcare policymakers, bureaucrats, regulators, managers, clinicians, patients and patient groups, researchers, and those in the specialized healthcare media—in fact, all those interested in how health systems work from the top to the bottom of the system, and in-between, and how they can be improved. We hope readers all gain something from this book and enjoy what follows. We believe there is no other offering like it. Some books on health reform or quality and safety involve OECD member countries but do not represent developing or under developed countries. Other books deal with health reform but not quality and safety; and yet others focus on quality and safety but not health reform. We, instead, are able to present a constellation of chapters from as wide a group of countries as we could obtain given space restrictions, each expressing their answer to the key question of whether big-scale health reforms affect quality and safety, and if so, how and to what extent.
Having documented what we did to get to this point, there is only one final suggestion to our readers. We invite you to immerse yourself in a treasure-trove of fascinating and skilled writing from a cross-section of countries of the world, documenting their trials and tribulations in reforming, and seeking to improve, the quality and safety of care to their citizens. In human endeavors, it is hard to discern a topic that is more important to the world’s present and future patients than to improve how health systems function.
PART I
Africa and Western Asia
We open our account with Part I, an examination of Africa and Western Asia. The countries involved are a mix of lower- and higher-income countries, providing contrasts in health systems, reform efforts, and quality and safety initiatives. The countries are Ghana, Israel, Oman, and South Africa. In addition, unusually, compared with the rest of the book, we have a single chapter in this part covering seven countries—the Gulf States. They are brought together as their safety and quality issues are coordinated through the Health Ministers’ Council in the Gulf Countries, involving efforts in Bahrain, Kuwait, Oman, Qatar, the Kingdom of Saudi Arabia, the United Arab Emirates, and the Republic of Yemen.
A key determinant of health governance and reform is per capita income. The wealth of the country is a major factor in the amount of resources available to provide for and pay the workforce, to build and maintain facilities and infrastructure, and tackle everything from basic community-level infections to child health, maternity service provision, and the like. Here we see the wide range of foci of the systems in this part, depending on those wealth differences. South Africa, a lower-income country, and Ghana, until recently relatively low, but now approaching middle-income levels, are both concerned with providing core services to the whole population, including dealing with issues of inadequate staffing and poor distribution of the workforce throughout the country, as well as tackling urgent problems such as maternal and child health, HIV/AIDS, and universal immunization.
Israel and Oman, with much more developed economies, are not lacking challenges; but in their cases many of the more fundamental issues facing South Africa and Ghana have been addressed. They, instead, can focus on figuring out how to tackle challenges such as improving the public availability of data, designing and introducing pay for performance models, and enhancing an already effective IT regime.
The chapter on the Gulf States nicely straddles this divide between rich and poor health systems, providing an interesting picture of how efforts are being coordinated across seven countries with widely disparate resource capabilities. Gross national income per capita in these states differs by a factor of almost 35—from $2,310 to $80,470 per person (purchasing power parity in international dollars). So across the Gulf countries, the problems differ enormously. Nevertheless, the Gulf States have recognized that there is much to be gained by sharing expertise, perspectives, and efforts in health reform and quality of care, and, as shown in the Gulf chapter in particular, there is much to learn in coordinating efforts and sharing ideas about creating safer systems and improved care for patients.
Chapter 2
Ghana
Abstract
For more than a decade, Ghana has embarked on a number of health sector reform initiatives. These reforms have been aimed at improving access to quality healthcare and reducing financial risk, especially to the poor and vulnerable. The expectation is that these will contribute to bridging equity gaps and improving health outcomes. Through an evaluation of current reform initiatives, we portray their overarching impact on quality and safety. A brief historical account of the health system and its organization, current reform initiatives and their impact, the quality and safety landscape, and the future direction are tackled.
A Brief History of Healthcare Reform in Ghana
At independence from British colonial rule in March 1957, Ghana, under President Kwame Nkrumah, introduced free medical care. This was funded through general taxation. It marked a departure from the out-of-pocket payment schemes that characterized the pre-independence era. Subsequently, following stagnating economic fortunes, the Government, in 1972 and 1985 respectively, introduced low, and later significant, out-of-pocket payments at the point of service. The objective was to address stock outs of essential medicines and supplies. The Government’s aim of a 15 percent recovery of recurrent expenditure in the 1985 out-of-pocket payment policy was achieved. This, however, introduced significant attendant inequities in access to care (Agyepong & Adjei 2008, Waddington & Enyimayew 1989). By 2000, and on the verge of national elections, public uproar against the out-of-pocket scheme, now christened “Cash and Carry,” had peaked. This led to the center-right opposition New Patriotic Party (NPP) pledging to replace it with a National Health Insurance Scheme (NHIS), which it did subsequently.
Table 2.1 Demographic, economic, and health information for Ghana
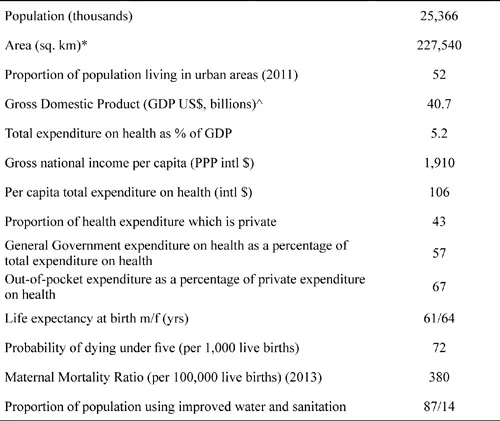
Source: Unless otherwise stated data are for the year 2012 and taken from the World Health Organization 2014a. * Area from the World Bank 2014a. ^ GDP from the World Bank 2014b.
Notes: PPP is purchasing power parity, intl $ is international dollar which has the same purchasing power as US$ in the US.
Another set of major reforms occurred with the introduction of the Ghana Health Service and Teaching Hospital Act (1996), Act 525 (Government of Ghana 1996). This, in fact, led to the formation of the Ghana Health Service (GHS), which then became an “autonomous Executive Agency responsible for implementation of national policies under the control of the Minister for Health through its governing Council” (Ghana Health Service 2014). Through a number of partnership arrangements, the Ministry of Health coordinates the actions of the GHS and other agencies like the Teaching Hospitals, the Christian Health Association of Ghana (CHAG), the private self-financing sub sector, non-governmental, and civil society organizations (Ghana Health Service 2014).
These reforms have allowed for a clear separation of the policy formulation, resource mobili...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Contents
- List of Figures
- List of Tables
- List of Contributors
- Acknowledgements
- Foreword by David W Bates and Clifford F Hughes
- 1 Introduction
- PART I AFRICA AND WESTERN ASIA
- PART II EASTERN ASIA AND SOUTHERN ASIA
- PART III SOUTH EASTERN ASIA AND OCEANIA
- PART IV THE AMERICAS
- PART V EUROPE
- References
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Healthcare Reform, Quality and Safety by Jeffrey Braithwaite,Yukihiro Matsuyama,Julie Johnson in PDF and/or ePUB format, as well as other popular books in Politics & International Relations & Health Care Delivery. We have over 1.5 million books available in our catalogue for you to explore.