Thyroid and Parathyroid Disorders in Children: A Practical Handbook offers a focused and practical approach to diagnostic and therapeutic (both medical and surgical) interventions in management of thyroid and parathyroid diseases in children. It is divided into two sections: thyroid and parathyroid, with each section discussing the use of the laboratory testing and radiographic modalities in the study of these glands. This guides the reader to know the utility and limitations of the findings when approaching a child with these conditions. Written by international experts in the fields of pediatric endocrinology and endocrine surgery, it is ideal for trainees, practicing physicians and professionals who care for children with endocrine conditions.
Key Features
Discusses differences in recognition and management of thyroid and parathyroid disorders in children compared with adults, with both common and rare disorders described along with their medical and surgical treatment techniques.
Aids the practicing physicians, endocrinologists, trainees, and fellows in understanding the complex concepts in a practical way.
Fills the gap in the market for a much-needed book concentrated on endocrine neck diseases of childhood.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Tests of antibodies associated with thyroid dysfunction
Limitations in common immunoassays
Biotin (vitamin B7)
Avoiding and correcting for immunoassay interference
Testing thyroid fine needle aspiration specimens
Molecular testing
References
Background
The hypothalamic–pituitary–thyroid (HPT) axis is responsible for the regulation and production of thyroid hormone (TH). The hypothalamus secretes thyrotropin-releasing hormone (TRH), which stimulates the pituitary gland to produce thyroid-stimulating hormone (TSH), which causes the production and release of thyroid hormones (TH). The two forms of TH are thyroxine (T4) and triiodothyronine (T3). When children present with symptoms of hypothyroidism, hyperthyroidism, goiter, or thyroid nodules, in addition to a thorough history and physical, they warrant assessment of the biochemical status of the HPT axis.
At this time, clinically available tests allow for measurement of the concentration of TSH, total T3, total T4, unbound or free T4 (FT4) and free T3 (FT3), and reverse T3. In addition, antibodies associated with thyroid pathology can be detected.
Available laboratory tests of thyroid function
In the majority of clinical situations, TSH and FT4 or total T4 will be sufficient to screen for common thyroid disorders such as hypothyroidism and hyperthyroidism (1). As with all tests, there can be false-negative and false-positive results. There are numerous reports in the literature describing cases in which patients were adversely affected by acting on inaccurate lab results. Before ordering or interpreting tests of thyroid function, clinicians should have an understanding of the limitations of these assays. Accurate measurement and interpretation are paramount to clinical care, and interest in this area is large. Between 1981 and 2017, over 100 articles were published discussing laboratory evaluation of thyroid status (2)! In this section, we will summarize the assays most common in clinical practice and their limitations.
When assessing thyroid function, lab tests can be categorized into those that assess the HPT axis: TSH, FT3, FT4, total T3, total T4, and reverse T3, and those that assess for autoantibodies that can affect thyroid function: thyroid peroxidase antibody (anti-TPO), thyroglobulin antibody (TgAb), and TSH receptor antibodies. TSH receptor antibodies can be inhibitory, stimulatory, or neutral. In the past, estimation of free TH concentrations relied upon resin uptake, FT4 index, and T4/thyroid binding globulin ratio (3). With increased availability and specificity of FT3 and FT4 testing, these prior tests are no longer recommended for first-line testing and they will not be discussed in this review.
Types of assays used
Immunoassays are the mainstay for measuring TSH and TH. Immunoassays rely upon a labeled antibody reacting with an analyte (such as TSH) of interest. Advantages of immunoassays include their ability to detect small amounts of analyte, lack of significant personnel oversight/participation, and quick time to result (2). As specificity of the labeled antibodies improved, so did the sensitivity of the assays. For example, the first generation TSH assays had a lower limit of detection of 1.0 mIU/L. The third generation TSH assays now have a detection of 0.01 mIU/L (1). Both biotin and streptavidin are commonly used in these immunoassays (2, 4, ), and this will become important when considering assay interference.
There are several forms of immunoassays relevant to thyroid evaluation:
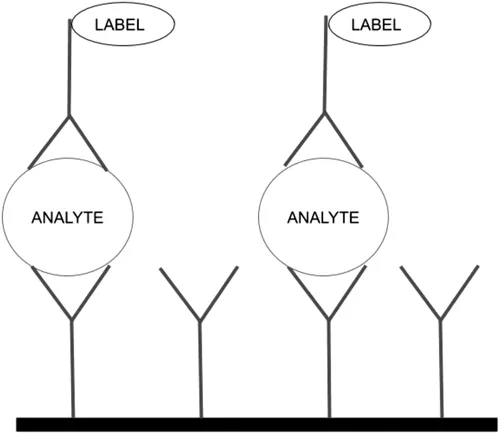
1. Sandwich immunoassay (also known as a two-site, non-competitive immunoassay): The patient’s serum is mixed with two antibodies. The “capture” antibody binds to one part of the analyte. The “labeled detector” antibody binds to another part of the analyte (1). The detector antibody measured is directly proportional to the amount of analyte present. See Figure 1.1.
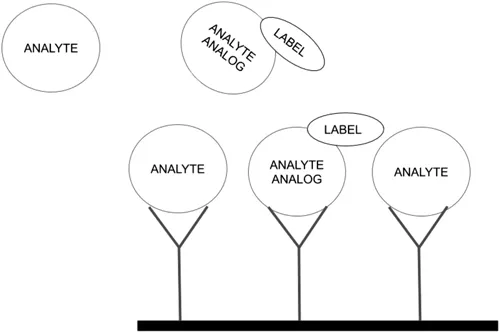
2. One-step competitive immunoassay: The analyte and labeled analyte analog compete for binding to the capture assay. The amount of signal (label) detected is inversely proportional to the amount of analyte present (1). See Figure 1.2.
3. One-step non-competitive immunoassay: A labeled antibody binds to the analyte. The sample is then washed, removing the unbound labeled antibodies. The amount of signal is directly related to the amount of analyte.
4. Bioassay: This is a functional assay used to check for the presence of stimulatory TSH receptor antibodies. The patient serum is mixed with cells designed to express the TSH receptor. If stimulatory antibodies are present, they stimulate the TSH receptor, causing increased production of cyclic AMP. The amount of cyclic AMP is then measured and is proportional to the amount of stimulatory TSH receptor antibodies (1, 5, ).
5. Bridge-immunoassay: This two-step assay relies upon the binding of TSH receptor antibodies to both an immobilized capture receptor and a signal receptor (1, 5, ). The TSH receptor antibody forms a “bridge” between the capture receptor and the signal receptor. The amount of signal measured is proportional to the amount of TSH receptor antibodies present.
Figure 1.1 Sandwich assay.
Figure 1.2 One-step competitive assay.
Measuring free hormone concentration: When measuring FT3 or FT4 concentration, one must consider the potential of measuring protein-bound T4 and T3 interacting with the capture antibody and impacting results. To reduce this, one can separate the protein-bound T3 and T4 from the FT3 and FT4 prior to measurement. The two ways to do this are ultrafiltration and equilibrium dialysis. In ultrafiltration, the sample is centrifuged and the ultrafiltrate is then measured (1). In equilibrium dialysis, there is a dialysis membrane which separates the small molecules (FT3 or FT4) from the larger molecules (proteins), allowing for direct measurement of free hormone concentrations (1).
Tests of antibodies associated with thyroid dysfunction
Thyroid peroxidase antibody (TPO-Ab): TPO-Ab is sensitive but not specific for Hashimoto’s thyroiditis (3). It is present in 5–20% of the general population with an incidence that increases with advancing age (6).
Thyroglobulin antibody (TgAb): Although TgAb can be tested when one is considering a diagnosis of Hashimoto’s thyroiditis, its main role has shifted from diagnosing autoimmunity to accurately assessing thyroglobulin in differentiated thyroid cancer survivors (3). When TgAb is present, it can interfere with thyroglobulin measurement, resulting in falsely low measurements (7). This interference can significantly complicate monitoring for disease recurrence. Regarding testing for Hashimoto’s thyroiditis, TgAb is found in up to 10% of healthy patients, including 6.3% of children aged 12–19 (6). When TgAb is present without co-current anti-TPO, there is no significant association with thyroid disease. In a study of 17,353 people aged 12–80+, not a single patient with hypothyroidism had a positive TgAb with a negative TPO-Ab (6).
TSH receptor antibodies (TRAbs): TRAbs can be stimulatory, inhibitory, or neutral. When testing for TRAbs it is helpful to not only test for presence or absence, but also test for biochemical effect. All TRAbs can be detected by competitive TSH-binding assays (3), but to specifically assess for the presence of stimulatory TRAbs, the specific thyroid-stimulating-immunoglobulin (TSI) bioassay is ideal (1, 3, 5, ).
Limitations in common immunoassays
All antibody-based immunoassays are subject to potential interference. At its worst, immunoassay interference has been known to lead to unnecessary interventions, including chemoth...
Table of contents
Cover
Half-Title
Title
Copyright
Dedication
Contents
Preface
Acknowledgments
Editors
List of Contributors
1 Laboratory evaluation of thyroid function
2 Imaging of the thyroid gland
3 Congenital hypothyroidism
4 Acquired hypothyroidism
5 Hyperthyroidism
6 Thyroid nodules
7 Thyroid cancer
8 Thyroid surgery
9 Laboratory evaluation of parathyroid gland function
10 Imaging of the parathyroid gland
11 Hypoparathyroidism in pediatric patients
12 Pseudohypoparathyroidism
13 Other genetic parathyroid conditions
14 Hyperparathyroidism
15 Parathyroid carcinoma
16 Parathyroid surgery in children
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Thyroid and Parathyroid Disorders in Children by Pallavi Iyer, Herbert Chen, Pallavi Iyer,Herbert Chen in PDF and/or ePUB format, as well as other popular books in Medicine & Endocrinology & Metabolism. We have over 1.5 million books available in our catalogue for you to explore.