This pocket-sized book, presented in an easy-to-follow format, is designed as a tool for students and professionals to carry in any setting, providing a quick reference guide to antenatal care and related anatomy and physiology. Used as a platform for wider reading, this text is an ideal reference point for any student or professional involved with the care of childbearing women.
- 78 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Antenatal Midwifery Skills
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineDrug administration
◼ Drugs and Midwives/Student Midwives
- All staff must adhere to the NMC Code 2015.
- Appropriate training must be undertaken to administer any drug.
- Qualified midwives can administer on their own initiative drugs on the Midwifery Exemptions list – see below and Trust lists.
- If trained and signed up for, qualified midwives can administer appropriate Patient Group Directives (PGDs) without prescription.
- Student midwives (regardless of any prior qualifications) can administer drugs on the Exemptions list only and only under direct supervision from a qualified midwife. This excludes drugs on the PGD list and controlled drugs, including pethidine, which need to be prescribed by an obstetrician.
- Drugs that were originally an exemption but were moved to the list of PGDs cannot be administered by a student midwife.
- Any drug not listed as an exemption or PGD must be prescribed by a medical practitioner.
- Administration of drugs must adhere to the local Trust policy.
◼ Midwives’ Exemptions and PGDS
The list provided below is of the most commonly used exemptions midwives can give during the course of their professional practice. The full list may be found in NMC (2019) Practising as a Midwife in the UK.
- Diclefenac
- Hydrocortisone Acetate
- Nystatin
- Phytomenadoione
- Diamorphine
- Morphine
- Pethidine hydrochloride
- Adrenaline
- Anti D immunoglobin
- Carboprost
- Cyclizine
- Ergometrine maleate
- Gelofusine
- Hartmann's solution
- Hepatitis B vaccine
- Lidocaine
- Naloxone hydrochloride
- Prochlorperazine
- Sodium Chloride 0.9%
◼ Safe Administration
Remember to check that the woman is not allergic to the drugs prescribed!
TEN RIGHTS | WHAT TO CHECK |
|---|---|
Right patient | Check wristband against drug chart. Confirm woman's name, date of birth and unit number |
Right medicine | Check packaging and date of expiry |
Right dose | Check dose of drug on packaging against prescription chart and calculate required amount (e.g. number of tablets) |
Right time | Check when previous dose was administered and check prescription chart |
Right route | Check that prescribed route is correct for the drug to be administered. Check that the woman is physically able to take the medication |
Right patient education | Check that the woman understands and inform of any side effects |
Right document | Is the drug prescribed and signed for? |
Right to refuse | Has the woman consented? (She is entitled to refuse) |
Right assessment | Check if drug is needed, baseline observations, contraindications |
Right evaluation | Has the medicine worked, are any further observations needed? |
◼ Drug Abbreviations
- BD – bis die, twice daily
- g – gram
- IM – intramuscular
- IV – intravenous
- Mané – morning
- mcg – microgram
- mg – milligram
- ml – millilitre
- Nocté – night
- OD – omni die, once daily
- PO – per oral
- PR – by rectum
- PRN – pro re nata, when required
- QDS – quater die sumendum, four times daily
- SC – subcutaneous
- SL – sublingual
- Stat – immediately
- Supp – suppository
- TDS – ter die sumendum, three times daily
◼ Formulas/Drug Calculations
Tablets/solutions
Intravenous infusions
The drop rate is found on the giving set.
Emergencies
◼ Adult Life Support for a Pregnant Woman
Figure 16Adult life support for a pregnant woman

Source: Based on information from the Resuscitation Council (UK) (2015) Resuscitation Guidelines, http://www.resus.org.uk.
◼ Antepartum Haemorrhage
Any amount of bleeding in pregnancy should be referred to the hospital.
Figure 17Management of an antepartum haemorrhage

◼ Eclampsia
Figure 18Management of eclampsia

If fits continue then the infusion should be stopped and a further slow bolus of 2gm IV given followed by the infusion again.
Check serum magnesium every 4–6 hours. Assess for signs of reduced respiration, oliguria, confusion. Ensure Calcium Gluconate 1gm IV is available as an antidote. Therapeutic level should be 2–4 mg/dL.
Female genital mutilation
There are four types:
- Type 1 – clitoridectomy: partial or total removal of the clitoris and possibly the prepuce.
- Type 2 – excision: partial or total removal of the clitoris and the labia minora, with or without excision of the labia majora.
Figure 19Degrees of female genital mutilation
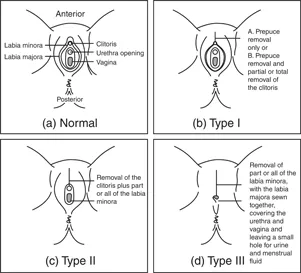
- Type 3 – infibulation: narrowing of the vaginal opening through the creation of a covering seal. The seal is formed by cutting and repositioning the inner, and sometimes outer, labia, with or without removal of the clitoris.
- Type 4 – other: all other harmful procedures to the female genitalia for non-medical purposes (e.g. pricking, piercing, incising, scraping and cauterising the genital area).
Women with type 3 will need referral to a specialist midwife for follow-up care and for deinfibulation if they wish to have a vaginal birth.
Functions of the placenta
- Respiration – absorbs oxygen and excretes carbon dioxide.
- Nutrition – glucose is stored as glycogen. Placental enzymes break down nutrients supplied by the mother.
- Excretion – fetal waste products are transferred back to the mother via the placenta.
- Protection – limited but prevents the passage of bacteria and enables maternal antibodies to pass to the fetus.
- Hormone production – (1) hCG to maintain the corpus luteum until the placenta is fully formed by about 12 weeks; (2) progesterone and oestrogen; (3) human placental lactogen for glucose metabolism.
Methods of induction
- Membrane sweep performed by midwife or obstetrician between 40 and 42 weeks' gestation.
- Artificial prostaglandin – pessary or gel – inserted into the posterior fornix of the cervix. Can take more than one dose to soften the cervix.
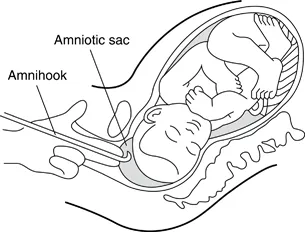
- Artificial rupture of membranes (ARM) using an amnihook. Requires the cervix to be effaced and dilated enough, and the presenting part to be engaged in the pelvis.
- Oxytocin intravenous infusion – commenced only after the rupture of membranes. Can induce contractions very quickly, so sufficient analgesia needs to be considered.
Figure 20Use of an amnihook
Minor disorders
| DISORDER | SUGGESTED MANAGEMENT/ADVICE |
|---|---|
Nausea and vomiting |
|
Table of contents
- Cover
- Title Page
- Copyright Page
- Contents
- LIST OF FIGURES
- LIST OF TABLES
- LIST OF ABBREVIATIONS
- ABDOMINAL EXAMINATION
- ANAEMIA
- ANATOMY
- ANTENATAL APPOINTMENTS
- ANTENATAL SCREENING
- BENEFITS
- BISHOP’S SCORE FOR INDUCTION OF LABOUR
- BLOOD PRESSURE TAKING
- BLOOD VALUES
- BMI
- BOOKING ADVICE
- BRITISH SIGN LANGUAGE
- CALCULATING ESTIMATED DELIVERY DATES
- CHOLESTASIS
- CTG INTERPRETATION
- CUSTOMISED GROWTH CHARTS
- DIABETES
- DRUG ADMINISTRATION
- VULNERABLE GROUPS OF WOMEN
- REFERENCES
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Antenatal Midwifery Skills by Alison Edwards in PDF and/or ePUB format, as well as other popular books in Medicine & Gynecology, Obstetrics & Midwifery. We have over 1.5 million books available in our catalogue for you to explore.