This comprehensive text provides practical approaches to adapting empirically supported treatments for eating disorders for clinicians working with patients of diverse backgrounds and presentations, or within non-traditional treatment settings across levels of care.
The book describes empirically- and clinically-informed treatment adaptations that impact delivery of real-world services for eating disorder patients and generate interest in testing adapted treatments in randomized controlled trials. Featuring contributions from researchers and clinicians with expertise in developing, delivering, and testing interventions for eating disorders, each chapter focuses on a specific population, setting, or training approach. Practical applications are then illustrated through case examples and wisdom gleaned through the contributors' own clinical studies and experiences.
Readers working with a diverse population of eating disorder patients will gain the necessary skills to support their patients on the journey to recovery and self-acceptance.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Adapting Evidence-Based Treatments for Novel Populations
1 Cultural Adaptations of Evidence-Based Treatments for Eating Disorders
Mae Lynn Reyes-Rodríguez and Debra Franko
Introduction
The tremendous growth of populations from diverse cultural backgrounds across the United States poses unique challenges for providing culturally competent care, particularly for mental health. According to the U.S. Census projections, it is expected that the U.S. population will become a majority–minority nation for the first time in 2043 (Colby & Ortman, 2014). Due to the new geographic composition, the use of the term “culturally sensitive” or “cultural competence” has increased in relevance in the mental health literature with the aim to address and reduce ethnic disparities in mental health care access and outcomes (Alarcon et al., 2009). Culture, context, and language are essential considerations for culturally competent care. The American Psychological Association provides guidelines as a way to educate psychologists about issues of diversity (APA, 2003). The importance of providing culturally sensitive practices and being well informed about culture, race, ethnicity, national origin, and language is not only an ethical issue, but also essential for the effective implementation of services or research (APA, 2017).
The literature on culturally sensitive treatments for eating disorders in the United States within diverse populations is limited. This is due, in part, to the misconception that eating disorders primarily affect White females from a specific socioeconomic background, and do not occur in other ethnic/racial groups; as a result, most treatment and assessment protocols have been developed primarily for Whites and may not be valid for use with other ethnic groups (Smolak & Striegel-Moore, 2001). Contrary to this misconception, it is well documented that eating disorders affect people from diverse ethnic and racial backgrounds (Franko, Becker, Thomas, & Herzog, 2007; Rodgers, Berry, & Franko, 2018; Udo & Grilo, 2018). Furthermore, functional impairment associated with a lifetime history of eating disorders is comparable or higher in diverse populations (i.e., Latinos, Asian Americans, and African Americans) as compared with non-Latino Whites (Marques et al., 2011). There is considerable need for understanding the complex interactions between race/ethnicity and the psychological factors that contribute to the development of eating disorders (Rodgers et al., 2018).
The research on ethnicity-based disparities in psychiatric diagnosis and access to care reflects three main issues that can lead to lack of appropriate treatment and impede access to care: (1) the poor fit of psychiatric diagnostic categories with ethnically diverse explanatory models and presentations of illness that could potentially lead to improper diagnosis (Alegria et al., 2008); (2) the differential help-seeking patterns for illness across racial/ethnic groups which requires different approaches to enhance engagement into treatment (Alegria et al., 2006); and (3) clinician error or bias due to the misperception that eating disorders are not prevalent in members of diverse populations. Culturally sensitive guidelines and protocols are suggested for potential modifications in the treatment content and delivery process that could affect outcomes by enhancing treatment effects, engagement, or retention and therefore reduce mental health disparities.
The purpose of this chapter is to provide the most updated information about culturally sensitive treatments for eating disorders for diverse populations. The first part of the chapter is devoted to defining what entails a cultural adaptation, discussing cultural adaptation frameworks, and determining when it is appropriate and necessary to integrate a culturally sensitive approach. The second part includes a review of research of culturally sensitive evidence-based treatments (EBTs) conducted with diverse populations in the United States. Finally, other relevant factors to take into consideration when working with diverse populations are discussed.
What is a Cultural Adaptation?
Cultural adaptation of treatments is one means for ensuring that EBTs that have been primarily developed and evaluated with study population representative of the majority culture are feasible, acceptable, and effective across diverse ethnic and social groups (Bernal, Jiménez-Chafey, & Domenech-Rodríguez, 2009; Domenech Rodríguez & Bernal, 2012). Dissonance can emerge when EBTs are applied untested in ethnic minority groups (Barrera & Gonzalez Castro, 2006). According to Bernal et al. (2009), cultural adaptation involves a systematic modification of an intervention to integrate clients’ relevant cultural factors (e.g., language and values). Whaley and Davis (2007) emphasized that the modification could be either in the content or in the delivery of an EBT or both, in order to accommodate values, attitudes, and practices of the target population.
Guidelines or systematic approaches for treatment adaptation in clinical trials and for the implementation of treatment in practice have been developed (APA, 2003). The DSM-5 Cross-Cultural Issues Subgroup developed a cultural formulation interview for implementation in diagnostic assessment to ensure that clinicians tap relevant domains of social, cultural, and ethnic identities (Alarcon et al., 2009). Furthermore, Griner and Smith (2006) made specific recommendations for the cultural modification of mental health interventions which emphasize the integration of the cultural values of the client in the therapy process (i.e., language, extended family, and spiritual traditions) and matching clients with therapists of the same race/ethnicity when possible. Bernal, Bonilla, and Bellido (1995) and Gonzalez Castro, Barrera, and Holleran-Steiker (2010) emphasized the importance of combining culturally adapted EBTs with culturally competent trained clinicians in the delivery of the intervention. Culturally adapted treatments appear to be especially valuable and acceptable to Latino individuals in the United States with low levels of acculturation (Griner & Smith, 2006).
Domenech Rodríguez and Bernal (2012) discussed ten models/frameworks and one guideline that have been published to address cultural adaptation of EBTs. Although there are some nuances among these models/frameworks, they concur that an initial exploratory phase, including gathering feedback from the target population and a literature review, should be the first step taken to inform the need for the cultural adaptation for the target population. Each model/framework emphasizes some specific steps of the cultural adaptation process with diverse levels of involvement of the target population but with the goal of providing a culturally sensitive approach congruent with the original EBT (Table 1.1).
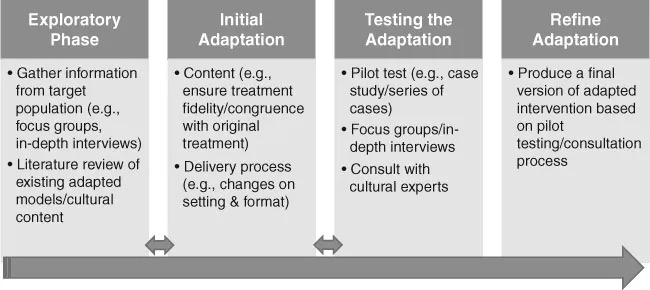
Although the need for culturally sensitive treatments is clear (Bernal & Domenech Rodríguez, 2009; Falicov, 2009), specific guidelines about when and how to conduct a cultural adaptation are not explicit in the literature (Domenech Rodríguez, Baumann, & Schwartz, 2011) and the implementation of standards is limited (Smith, Domenech Rodríguez, & Bernal, 2011). Gonzalez Castro et al. (2010) summarized four basic conditions to justify a cultural adaptation: ineffective patient engagement; unique risk or resilience factors in a subcultural group; unique symptoms of a common disorder that the original EBT was not designed to influence; and poor intervention effectiveness with a particular subcultural group. Figure 1.1 summarizes the basic steps for a cultural adaptation process.
Brief Review of Existing Literature
Prevalence Studies
Eating disorders, disordered eating, unhealthy weight control behaviors, and body image concerns are well documented among racially and ethnically diverse individuals across the United States and around the world (Reyes-Rodríguez et al., 2010; Rodgers et al., 2018; Sinha & Warfa, 2013). While current stereotypes that eating disorders only affect affluent White females remain (Sonneville & Lipson, 2018), the scientific literature is replete with empirical data and epidemiological studies providing ample evidence to support dismissing this common stereotype (Blostein, Assari, & Caldwell, 2017; Perez, Ohrt, & Hoek, 2016; Rodgers et al., 2018; Swanson, Crow, Le Grange, Swendsen, & Merikangas, 2011). We begin this section with a very brief review of robust epidemiologic studies.
Table 1.1 Frameworks, Models, and Guidelines for Cultural Adaptation of Evidence-Based Treatments
Name
Year
Authors
Key Elements
The Multidimensional Model for Understating Culturally Responsive Psychotherapies (Framework)
1992
Koss-Chioino and Vargas
Two dimensions: (1) culture (context and context); and (2) structure (process and form)
Three steps: (1) cultural gaps are identified; (2) literature review to inform the content that will fill the gap; and (3) testing the intervention to improve validity
Cultural Sensitivity Framework
2002
Resnicow, Soler, Braith-waite, Ahluwalia, and Butler
Two dimensions: (1) surface (appearance); and (2) deep (contextual influences on behaviors)
Cultural Adaptation Process Model
2004
Domenech-Rodríguez and Wieling
Three phases: (1) setting the stage; (2) initial adaptations; and (3) adaptation iterations
Hybrid Prevention Program Model
2004
González Castro, Barrera, and Martinez
Three dimensions: (1) cognitive information processing; (2) affective motivational characteristics; and (3) environmental characteristics
Selective and Directed Treatment Adaptation Framework
2006
Lau
Adaptation would target: (1) engagement or (2) treatment outcomes, or both.
Heuristic Framework
2006
Barrera and González-Castro
Four steps: (1) gather information; (2) make preliminary adaptations to the intervention; (3) test the preliminary adaptations; and (4) refine adaptations
Culturally Specific Prevention (Framework)
2006
Whitbeck
Five stages: (1) search for existing research models; (2) existing research of ethnic minorities is reviewed; (3) engaging in cultural translation of key risk and protective factors; (4) unique cultural risk and protective factors are identified and measured; and (5) undertake culturally specific interventions trials and assessments
Integrated Top-Down and Bottom-Up Approach to Adapting Psychotherapy (Model)
2006 and 2009
Hwang
Six domains: (1) dynamic issues and cultural complexities; (2) orientation; (3) cultural belief; (4) client-therapist relationship; (5) cultural differences in expression and communication; and (6) cultural issues of salience
Adaptation for International Transport (Guidelines)
2008
Kumpfer, Pinyuchon, Teixiera de Melo, and Whiteside
Implemented in 17 countries focused on cultural adaptation but keeping treatment fidelity
Figure 1.1 Summary of Cultural Adaptation Process.
In a large nationally representative comparative study in the United States, Marques et al. (2011) found that in a sample of Latino/as, African Americans, Asian Americans, and Whites, the prevalence of anorexia nervosa (AN) and binge eating disorder (BED) was similar across all four of these groups. However, both lifetime and 12-month prevalence of bulimia nervosa (BN) was higher in Latino/as and African Americans relative to Asian Americans and Whites. In contrast to Whites, lifetime prevalence of “any binge eating” was higher and mental health service utilization was lower in all the three minority groups. Using a subset of the same nationally representative sample, Taylor et al. (2013) studied 5,191 adults and 1,170 adolescents who were either African American or Caribbean Black and found that while the lifetime prevalence of AN and BN was low (0–1.98%, depending on diagnosis ...
Table of contents
Cover
Half Title
Title Page
Copyright Page
Contents
List of Figures, Tables, and Boxes
About the Editors
List of Contributors
Acknowledgments
Preface
PART I Adapting Evidence-Based Treatments for Novel Populations
PART II Applying Evidence-Based Treatments in Nontraditional Treatment Settings
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Adapting Evidence-Based Eating Disorder Treatments for Novel Populations and Settings by Christina C. Tortolani, Andrea B. Goldschmidt, Daniel Le Grange, Christina C. Tortolani,Andrea B. Goldschmidt,Daniel Le Grange in PDF and/or ePUB format, as well as other popular books in Psychology & Family Medicine & General Practice. We have over 1.5 million books available in our catalogue for you to explore.