Background: Catheter ablation has become a widely used approach to treating various cardiac arrhythmias. Traditionally, catheter ablation procedures are guided by fluoroscopic imaging to help understand catheter position during mapping. The potentially significant exposure to radiation to the patient, physician, and staff increases risks of radiation exposure-related disease. Also, the protective lead garments worn increases risks of orthopedic injury. Current advanced electroanatomic mapping and intracardiac echocardiography technology have allowed the development of endocardial catheter ablation techniques without the use of fluoroscopy safely and effectively. A host of expert and experienced authors present a practical overview of the rationale and methodology for a low- or zero-fluoro environment in the electrophysiology lab with the critical goal of significantly reducing radiation exposure to the patient, physician, and staff.This practical guide: Covers the entire spectrum of commonly (and less commonly) performed ablation procedures via endocardial approach. Discusses general principles that are applicable across ICE and EAM platforms. Will assist the electrophysiologist and their team to safely and effectively work toward the significant reduction in fluoroscopy utilization while also likely improving procedural safety, i.e., fewer complications, after the adoption of these techniques. Includes a library of 50 videos, with 9 extended films (108 minutes) by Dr. Razminia detailing step-by-step procedures and techniques.
eBook - ePub
Fluoroscopy Reduction Techniques for Catheter Ablation of Cardiac Arrhythmias
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Fluoroscopy Reduction Techniques for Catheter Ablation of Cardiac Arrhythmias
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Section 1
Basis of Imaging in the
Electrophysiology Lab
Electrophysiology Lab
1
Radiation Safety in the Electrophysiology Lab
Kristen Breedlove, MPAS, PA-C; John Clark, MD
Introduction
Present-day fluoroscopy has its roots in the late 19th century. The risks of radiation were not known at the outset. In the subsequent 120 years, we have learned much about both the benefits of medical radiation, as well as the risks. This chapter will outline some of the history of the radiation risks, as well as protective measures that can be used to keep both the patient and the staff safe.
The 2 people primarily responsible for the birth of the modern day cath lab are Wilhelm Roentgen and Thomas Edison. In November 1895, Roentgen discovered x-rays while experimenting with various elements within electrified vacuum tubes. He observed that barium platinocyanide, painted on a piece of cardboard, would fluoresce when the cathode tube was electrified with an aluminum window in it. He called the new rays “x” rays, x being the mathematical symbol for “unknown.” While positioning various elements between the cathode ray tube and the fluorescent screen, he noticed that when his hands came between the 2, he could see the bones in his hands. Two weeks later, still experimenting with the new form of radiation, he took the first human radiograph of his wife Bertha’s hand (Figure 1.1).
When Bertha saw the bones of her hand and wedding ring, she is reported to have exclaimed, “I have seen my death!” If the quote is in fact true, then it was prescient, because she did later succumb to radiation-induced sarcoma.

Figure 1.1The first human radiograph: Bertha Roentgen’s hand.
Very soon after Roentgen discovered x-rays, Thomas Edison began his own experiments. By painting barium platinocyanide on the inside of a cardboard box built to fit over his eyes and block out any ambient light, he was able to visualize human bones in real time (Figure 1.2). His system was extremely simple and quite elegant. It is very much like a popular virtual reality system of today (Figure 1.3).
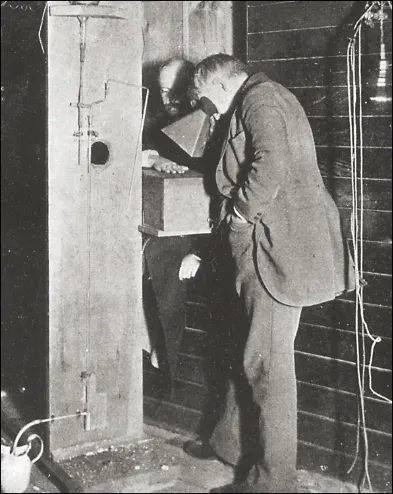
Figure 1.2Thomas Edison viewing Clarence Daily’s hand through an early fluoroscope.
Edison was one of the first to recognize the danger of x-rays. He himself suffered cataracts, which impaired his vision, and his lab assistant, Clarence Dally, suffered radiation dermatitis, which progressed to a fatal malignancy. Many of the early workers in x-ray research labs would later develop fatal malignancies. This group of workers became known as “x-ray martyrs.” In the late 1890s, the risk of an x-ray worker becoming an x-ray martyr was as high as 25%.1 By the early 1900s, the risk had dropped to about 1% to 2%.
Radiation-Associated Risks
Today, we recognize 2 types of radiation risk: deterministic and stochastic. Deterministic risks are dose-dependent. Below a threshold dose, the effect is not seen. Above the threshold, the severity is dose dependent, with higher doses resulting in worse injury. Deterministic risks include dermatitis, hair loss, and cataracts. Stochastic effects have no threshold level for occurrence. A greater dose will confer a greater risk, but any dose conveys some risk. While the odds of the complication occurring are dose dependent, the severity of the complication is independent of dose. Ionizing radiation causes creation of hydroxyl radicals within cells. The hydroxyl radicals can then ionize DNA base pairs, which lead to DNA strand breaks. Stochastic effects are related to this DNA damage. The DNA base pairs are usually repaired at the molecular level. If the damage is not repaired, the long-term risks of malignancy or birth defects may be seen. The risk is cumulative and lifelong. Young patients, since they have a longer remaining lifespan and greater chance of further radiation exposure, are at greater risk of stochastic effects. For the same dose of exposure, a child’s risk can be as much as 4 times greater than an adult’s.2

Figure 1.3Girl viewing her hand in a virtual reality system.
Malignancy Risk
The risk of malignancy from a single ablation procedure is small, but not zero. Many studies over the years have attempted to quantify it. Kovoor et al. measured radiation doses using thermoluminescence dosimeters in 9 adult females undergoing supraventricular tachycardia (SVT) ablation.3 From the radiation doses measured, they estimated a lifetime added risk of fatal malignancy of 0.03% for every 60 minutes of fluoroscopy. Perisinakis, using similar methods, estimated a risk of 0.065% malignancy from 60 minutes of fluoroscopy, and a risk of genetic defects of 1:1,000,000.4 Lickfett et al. reported a malignancy risk of 0.07% for women, and 0.1% for men for 60 minutes of fluoroscopy in their lab.5 So the realistic risk is likely to lie somewhere in the range of 1:1,000 to 1:5,000 for routine SVT ablations.
Deterministic Risks
The most common deterministic risks are cataracts, hair loss, and radiation-induced dermatitis. For the patient, the most likely deterministic risk is dermatitis. Given the technology of today’s fluoroscopy equipment, one might expect that radiation dermatitis never occurs. Surprisingly, there are many case reports in the literature, even as recently as 2018.6-10 The diagnostic clues to radiation dermatitis are a geometric rash, usually round or rectangular, arising 1 to 8 weeks after a radiologic procedure. Figure 1.4 shows a typical example.

Figure 1.4Radiation dermatitis.
Findings typically seen on histology include epidermal atrophy, dermal sclerosis, dilated superficial blood vessels, and atypical stellate fibroblasts. Malignant transformation into squamous cell or basal cell carcinoma can be seen. The threshold for development of dermatitis is about 5 Gy. If a patient receives a total dose >10 Gy, they should have follow-up to screen for dermatitis. If found, they should have close follow-up and possible surgical intervention due to the risk of malignant transformation. Biopsy is not usually indicated due to poor healing of the affected area.
Indirect Exposure Risks
While p...
Table of contents
- Cover
- Title Page
- Copyright Page
- Dedication
- Contents
- Contributors
- Forewords
- Preface
- Abbreviations
- Video Descriptions
- Section 1: Basis of Imaging in the Electrophysiology Lab
- Section 2: Ablation of Supraventricular Tachycardia
- Section 3: Ablation of Atrial Fibrillation
- Section 4: Ablation of Ventricular Arrhythmias
- Section 5: Special Populations
- Author Disclosures
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Fluoroscopy Reduction Techniques for Catheter Ablation of Cardiac Arrhythmias by Mansour Razminia, Paul C. Zei, Mansour Razminia,Paul C. Zei in PDF and/or ePUB format, as well as other popular books in Medicine & Cardiology. We have over 1.5 million books available in our catalogue for you to explore.