This is the second and updated version of the Textbook of Allergy for the Clinician. It is a unique book in the field of allergy. The uniqueness lies in the international character of the book with contributors representing both the East and West. This book represents the diversity of issues affecting patients in the specialty of allergy, asthma & immunology. There is some discussion of the basic mechanisms involved and extensive elaboration for the clinicians. This book will appeal to medical students, residents and fellows undergoing training as well as consultants in academic and clinical practice settings. The color plates, especially in the section on Aerobiology, will help in the interaction between the patient and consultant in identifying the plant or flora which is the causative factor. The differences and similarities between the Eastern and Western approaches in the practice of the specialty are being addressed for the first time in a book.
eBook - ePub
Textbook of Allergy for the Clinician
- 430 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Clinical Medicine1
Basics of Allergy
Immunological and Clinical
1 Division of Allergy and Immunology, National Jewish Health & University of Colorado, Denver. Colorado. USA. Email: [email protected]
2 Division of Allergy and Immunology, National Jewish Health, Denver. Colorado USA, Email: [email protected]
* Corresponding author: [email protected]
INTRODUCTION
The immune system is composed of an adaptive immune system and an innate immune system. The adaptive immune system distinguishes itself from the innate system by the following features: (a) Specificity of antigen recognition, (b) Diversity of the antigen receptor repertoire, (c) Rapid clonal expansion, (d) Adaptiveness to the changing environment and (e) Immunological memory. The innate system lacks fine specificity, has limited diversity and rudimentary memory but manifests rapid engagement. Lymphocytes are the primary cells of adaptive immunity; they include T cells, B cells and NK cells. Each individual cell type will be described in this chapter.
Lymphoid cell generation
Generation of Antigen-specific Receptors: The growth of B and T cells from pluripotent stem cells requires successive differentiation through a series of stages that starts in the bone marrow and ends in the thymus (T cells) or peripheral lymphoid tissue (B cells) (Marrack et al. 2000, Carding et al. 2002, Calame 2001). During differentiation lymphocytes are able to recognize self and non-self antigens through the expression of antigen-specific receptors known as T Cell Receptors (TCR) and B Cell Receptors (BCR) (Nemazee 2000). TCRs are comprised of ab or gd subunits whereas BCRs are composed of membrane-bound immunoglobulins (Fig. 1.1). Approximately 90% of peripheral blood T cells are ab+ and the remainder cells are gd+, although the proportion of the latter reaches 25–30% in the gastrointestinal mucosa and skin.2 The generation of TCRs and BCRs creates an impressive repertoire in the order of > 1014 through combinatorial joining of V, D and J (b and d chains) or V and J (Fig. 1.2). Recombination is triggered by IL-7 and involves recombination-activating gene-1 and -2 (RAG-1 & -2) and a DNA repair enzyme (metallo-b-lactamase) encoded by the gene Artemis (Hesslein and Schatz 2001). The deficiency of the RAG enzymes, IL-7 receptor- and the Artemis gene product causes Severe Combined Immunodeficiency (SCID). A partial deficiency of RAG-1 & -2 causes Omenn syndrome. The BCR is capable of recognizing small and large peptides, in contrast, the TCR recognizes small stretches of linear peptides of 10–12 amino-acids in length.
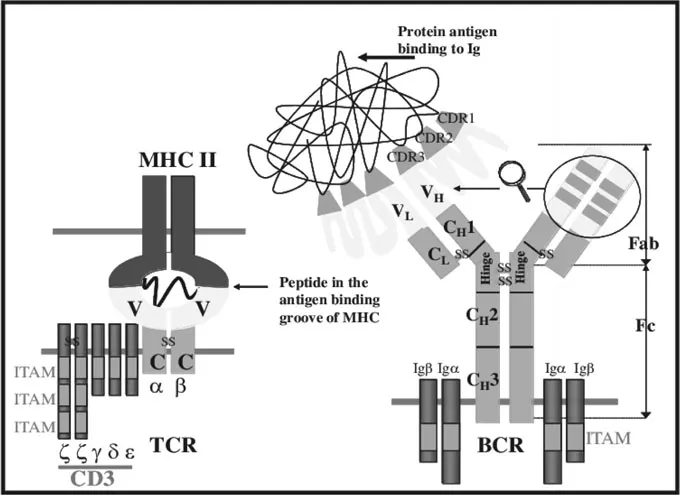
Figure 1.1. The composition of the T cell receptor (TCR) and the B cell receptor (BCR). TCR is composed of the CD3 complex and ab (or gd) subunits. ab (or gd) subunits bind the MHC-bound antigenic epitope, the CD3 complex transduces intracellular signaling. BCR is composed of the surface immunoglobulin and the Iga and Igb accessory molecules. MHC: Major histocompatibility complex; V: variable region of the receptor; C: constant region of the receptor; z z g d e are subunits of the CD3 complex; a and b are TCR subunits; Ig: membrane-bound immunoglobulin; Iga and Igb are BCR accessory BCR molecules; Hc and Lc are constant regions of the heavy (H) or light (L) chain of immunoglobulin; Hv and Lv are variable regions of the heavy (H) or light (L) chain of immunoglobulin; CDR: complementarity determining region.
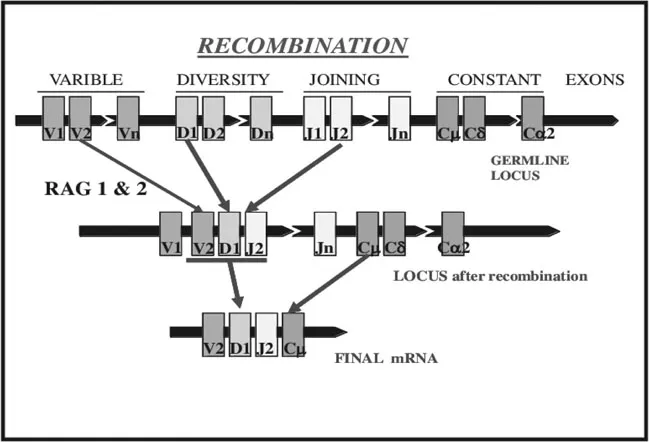
Figure 1.2. The immunoglobulin heavy chain locus as the example of genomic organization of antigen receptors. V, D, J exons encode the variable region of the immunoglobulin antigen-binding site and C exons encode the constant region.
Thymic Selection of T Cells: During the generation of antigen receptors, self MHC-reactive and non-reactive TCRs are generated (Hennecke and Wiley DC 2001).
T cells require signaling through the TCR for survival and proliferation; T cells that are unable to recognize self-MHC or have very low avidity TCRs for self-MHC die because of the lack of the TCR signal (death by neglect). T cells, which recognize self-MHC in conjunction with the self-peptide, are expanded (positive selection). Positively selected T cells with very high avidity for self-peptides (auto-reactive T cells) are killed (negative selection). Ninety-five percent of T cell precursors die due to negative selection/failing to express the appropriate TCR.
B cell precursors are not subjected to extensive deletions; self-reactive B cells undergo another round of receptor gene rearrangement (receptor editing) to replace an auto-reactive BCR with a normal BCR. In the early phase of differentiation, immature T cells express both CD4 and CD8 co-receptors (double-positive cells) (Sebzda et al. 1999, Germain 2002) CD4 T cells are selected through interaction with class II MHC molecules and CD8 T cells through interaction with class I MHC molecules.
Two tyrosine kinases—Lck (Lymphocyte-specific protein tyrosine kinase) and ZAP70 (zeta-associated protein 70) play a critical role in the selection of CD4 and CD8 T cells, respectively. Patients with congenital deficiency of Lck have severe combined immunodeficiency because of the failure of CD4 differentiation; ZAP70 deficiency results in a severe defect of CD8 T cell differentiation. A small fraction of T cells, mostly of gd subtype, is negative for both CD4 and CD8 (double negative) (Carding et al. 2002).
Immune surveillance—naïve lymphocyte
In order to increase the probability of antigen encounter, lymphocytes continuously circulate across various tissues. Naïve T and B cells preferentially migrate to lymph nodes due to homing receptors L-selectin and CCR7 (Moser and Loetscher 2001). Their ligands, CCL19 and CCL21 are expressed on High Endothelial Venules (HEV) of lymph nodes.
Events following an antigen encounter
Antigen Presentation: Professional Antigen Presenting Cells (APC) are those that express high levels of class II MHC molecules and possess the capacity to internalize, process and present foreign antigens in the MHC groove. APC cells include Dendritic Cells (DC), B cells, monocytes/macrophages and their tissue counterparts. Immature DCs, residing in the peripheral tissue, phagocytose and process foreign antigens (Table 1.1) (Guermonprez et al. 2002). Pathogen-derived molecules and cytokines from inflamed tissue, trigger DC maturation, enhance antigen processing and expression of foreign-peptide-loaded MHC proteins. Mature DCs secrete cytokines and upregulate different co-stimulators and CCR7.
| MHC I | MHC II | |
|---|---|---|
| Genes | HLA-A, B, C | HLA-DP, DQ, DR |
| Structure | Transmembrane a chain bound to b2-microglobulin, only the a chain interacts with the peptide | Transmembrane a and b chain, both chains interact with the antigenic peptide |
| Presented peptide | Peptides derived from self/non-self intracellular proteins, e.g., viral peptides | Peptides derived from extracellular proteins, e.g., bacterial peptide |
| Mechanism of presentation | Intracellular proteins are degraded by the ubiquitin/proteasome pathway in the cytosol; transported by TAP to endoplastic reticulum and loaded onto MHC; the MHC/peptide complex translocates to the cell membrane | Extracellular proteins are endocytosed and degraded by lysosomal proteases; subsequently peptides-containing endosomes are fused to MHC-containing vesicles; peptides are loaded onto MHC and the complex translocates to the cell membrane |
| Presenting Cells | All nucleated cells, including APC | Antigen Presenting Cells (APC): dendritic cells, B cells, macrophages |
| Interacting T cell | CD8 T cell | CD4 T cell |
| Receptor | Expression | Ligand | Role | Knock-out mice |
|---|---|---|---|---|
| CD28 family members | ||||
| CD28 | C constitutive | B7.1(CD80)I inducible (though CD40 stimulation), B7.2 (CD86) constitutive onAPC | E essential for initiat... | |
Table of contents
- Cover
- Title Page
- Copyright Page
- Dedication
- Foreword
- Preface
- Acknowledgements
- About the Sponsor
- Contents
- 1. Basics of Allergy: Immunological and Clinical
- 2. Immunology of Allergic Diseases
- 3. History Taking: Evaluation of Allergic Disorders
- 4. Allergy Skin Testing
- 5. In vitro Laboratory Tests for the Diagnosis of Allergy
- 6. Aerobiology for the Clinician: Basic and Applied Aspects, Pollen Sources, Pollen Calendars
- 7. Risk Factors for Allergies and Asthma
- 8. Rhinitis: Allergic and Nonallergic
- 9. Chronic Rhinosinusitis, Nasal Polyps and Aspirin Exacerbated Respiratory Disease
- 10. Allergic Diseases of the Eye
- 11. Rhinolaryngoscopy for the Allergist
- 12. Pediatric Asthma
- 13. Adult Asthma
- 14. The Pharmacotherapy of Rhinitis and Asthma
- 15. Allergen Immunotherapy
- 16. Pulmonary Function Testing
- 17. Common Office Tests and Procedures for the Allergist
- 18. Environment and Lifestyle in Allergic Disease
- 19. Effects of Air Pollution on Allergy and Asthma
- 20. Asthma and COPD—Similarities and Differences
- 21. Occupational Asthma
- 22. Anaphylaxis
- 23. Insect Venom Allergy
- 24. Urticaria and Angioedema
- 25. Atopic Dermatitis
- 26. Contact Dermatitis
- 27. Food Allergy—Introduction, Epidemiology, Pathogenesis and Clinical Presentation
- 28. Food Allergy—Diagnosis and Management
- 29. Immunodeficiency Diseases
- 30. Integrative Allergy and Asthma for Traditional Practice
- 31. Ayurveda and Yoga Therapy for Allergy and Asthma
- 32. Yoga Breathing Techniques in Asthma
- 33. Drug Allergyr
- 34. Latex Allergy
- 35. Allergy–Asthma Practice: East vs West
- Index
- About the Editors
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Textbook of Allergy for the Clinician by Pudupakkam K. Vedanthan, Harold S. Nelson, Shripad N. Agashe, PA Mahesh, Rohit Katial, Pudupakkam K. Vedanthan,Harold S. Nelson,Shripad N. Agashe,Rohit Katial,PA Mahesh, Pudupakkam K. Vedanthan, Harold S. Nelson, Shripad N. Agashe, Rohit Katial, PA Mahesh in PDF and/or ePUB format, as well as other popular books in Medicine & Clinical Medicine. We have over 1.5 million books available in our catalogue for you to explore.