- 248 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Concise Dermatology
About this book
As the comprehensive textbooks of Dermatology grow longer and more specialized, there is a need for a text to cut the subject back to the essentials a medical professional needs to know. This concise text from an internationally respected editor presents the most important points about the most significant topics in disease of the skin, hair, and nails; any medical professional will find here the material for a solid grounding in the subject.
*Covers the range of dermatology in a consistently manageable level of detail
*Answers the need for a reliable concise guide for medical professionals in all specialties
*Offers a straightforward and approachable synopsis of the subject
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
Topic
MedicineSubtopic
Diseases & Allergies1
An introduction to skin and skin disease
An overview
The skin is an extraordinary structure. It has a surface area of 2 m2 and accounts for 16–20% of the total body weight. It is made up of several types of tissues that work in harmony with one another (Figure 1.1). The large number of cell types and functions of the skin and its proximity to numerous potentially damaging stimuli in the outside environment result in two important consequences. The first is that the skin is frequently damaged because it is right in the ‘line of fire’, and the second is that each of the various cell types that it contains can ‘go wrong’ and develop degenerative and neoplastic disorders. Knowledge of the structure and functions of the skin is important for the clinician to diagnose and treat dermatological conditions.
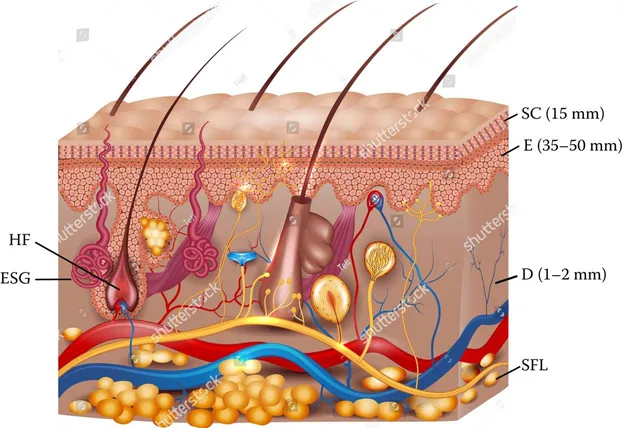
FIGURE 1.1 Structure of the skin: HF, hair follicle; ESG, eccrine sweat gland; SC, stratum corneum (15 mm); E, epidermis (35–50 mm); GCL, granular cell layer; ML, Malpighian layer; BL, basal layer; D, dermis (1–2 mm); SFL, subcutaneous fat layer.
Skin diseases are quite common, and almost every individual suffers from skin disease at least once in his or her lifetime. Atopic dermatitis affects about 15% of the people under the age of 12, while psoriasis affects 1–2%. Other conditions that affect a significant number of people are viral warts, seborrhoeic warts, and solar keratoses. It should be noted that 10–15% of the family physician’s work is with skin disorders, and that skin diseases are the second most common cause of time taken away from work. Although skin diseases are not uncommon at any age, they are particularly frequent among the elderly. The older one gets, the greater the risk of developing skin disease.
Skin disorders are not usually fatal but can cause considerable discomfort and disability. The disability caused can be physical, emotional, and socioeconomic. Patients receive help when their problems and disabilities are acknowledged and their physician makes attempts to address their various problems.
Skin structure and function
It is difficult to understand abnormal skin and its vagaries without understanding the composition and function of normal skin. Although, at the first glance, the skin may appear quite complicated, a slightly deeper look shows that there is an elegant logic behind its architecture, which helps it perform several vital functions. The skin is composed of epithelial and adipose tissues. The epithelial tissue comprises the epidermis and the dermis. The adipose tissue, on the other hand, contains the hypodermis. The accessory structures include hairs, nails, sebaceous, sweat glands, sensory receptors, etc.
The skin surface
The skin surface is a barrier between living processes and the potentially injurious outside world. Thus it plays the important role of preventing and controlling interactions between the outside and the constant and vulnerable inside. Its 2 m2 area is modified regionally, which enables it to better perform particular functions. The skin on the limbs and the trunk is very much the same, but the skin on the palms and soles, facial skin, scalp skin, and genital skin differ somewhat in structure and function. The surface is thrown up into a number of intersecting ridges, which make rhomboidal patterns. There are ‘pores’ at regular intervals opening onto the surface – these are the openings of the eccrine sweat glands. The diameter of these openings is approximately 25 μm, and there are approximately 150–350 duct openings per square centimetre (cm2). The hair follicle openings can also be seen at the skin surface and the diameter of these orifices and the numbers per cm2 vary greatly between anatomical regions. A close inspection of the follicular opening reveals a distinctive arrangement of the stratum corneum cells around the orifice.
At magnifications of 500–1000 times, which is possible with scanning electron microscopy (SEM), individual horn cells (corneocytes) can be seen in the process of desquamation (Figure 1.2). Corneocytes are approximately 35 μm in diameter, 1 μm thick and shield-like in shape.

FIGURE 1.2 Scanning electron micrograph of stratum corneum shows a corneocyte in the process of desquamation (from Marks and Motley, Common Skin Diseases, 18th edition, with permission).
The stratum corneum
Also known as the horny layer, this structure is the differentiated end-product of epidermal metabolism (also known as differentiation or keratinization); the final step in differentiation is the dropping off of individual corneocytes in the process of desquamation seen in Figure 1.2. The stratum corneum is composed of 20–25 layers of cornified cells (keratinocytes), which appear as flat cells and do not possess any nuclei or cytoplasmic organelles. The keratinocytes contain soft keratin. Lamellar bodies are important structures present around these keratinocytes. Lipids are released from the lamellar bodies, and these lipids contribute to the permeability of stratum corneum.
The corneocytes are joined together by the lipid and glycoprotein of the intercellular cement material and by the vestiges of the desmosomes that are well developed in the keratinocytes of the epidermis (see later). In the stratum corneum, they are known as ‘corneo-desmosomes’. The orderly release of corneocytes at the surface in the process of desquamation is not completely characterized, but it appears to depend on the dissolution of the corneo-desmosomes near the surface by a cascade of enzymes, their activators, and inhibitors, known collectively as ‘chymotrypsin’, which is activated by the presence of moisture. On limb and trunk skin, the stratum corneum is some 15–20 cells thick and, as each corneocyte is about 1 μm thick, it is about 15–20 μm thick in absolute terms. The stratum corneum of the palms and soles is about 0.5 μm thick and is, of course, much thicker than that on the trunk and limbs.
The stratum corneum prevents water loss, and when it is deranged, as, for example, in psoriasis or eczema, water loss is greatly increased so that severe dehydration can occur if enough skin is affected. It has been estimated that a patient with erythrodermic psoriasis (involvement of more than 90% body surface area) may lose 6 L of water per day through the disordered stratum corneum, in contrast to 0.5 L lost normally per day.
The stratum corneum also acts as a barrier to the penetration of chemical agents with which the skin comes into contact with it. It prevents systemic poisoning from skin contact, although it must be realized that it is not a complete barrier and percutaneous penetration of most agents does occur at a very slow rate. Those responsible for formulating drugs in topical formulations are well aware of this rate-limiting property for percutaneous penetration of the stratum corneum and try to find agents that accelerate the movement of drugs into the skin. In recent years, as more knowledge has been acquired about the penetrability of the stratum corneum and the pharmacokinetics of drugs, techniques have been developed for the administration of drugs systemically via the skin – the transdermal route.
The barrier properties also prevent microbial life invading into the skin; however, the barrier properties are not perfect, and, occasionally, pathogen gains entry via hair follicles or small cracks and fissures and causes infection. Antimicrobial peptides – the cathelicidins – also play an important role and some function at the stratum corneum level.
The structure of the stratum corneum is very extensible and compliant in health, permitting movement of the hands and feet, and is actually quite tough, thus providing a degree of mechanical protection against minor penetrative injury. The ability to extend is greatly aided by the system of skin surface markings (varying by the region sampled), which take the form of rectangles and behave like ‘concertinas’ when stretched. The various functions of the skin have been summarized in Table 1.1.
TABLE 1.1
Functions of the skin
Barrier function |
| •Permeability barrier to water and electrolytes •Prevention of entry of microbes and chemicals •Protection from ultraviolet rays •Prevention of injury due to blunt objects |
Maintenance of body temperature |
Sensory functions |
•Mechanoreceptors (touch, vibration, pressure) •Thermoreceptors (heat and cold) •Nociceptors (pain and itch) •Free nerve endings •Corpuscular receptors |
Immunological functions |
Synthesis of vitamin D and E |
Transport of nutrients and metabolites |
Sexual attraction |
The epidermis
The epidermis mainly contains keratinocytes; but it also contains non-keratinocytes – melanocytes and Langerhans cells, both of which possess dendrites. This cellular structure is some three to five cell-layers thick, on average, 35–50 μm thick in absolute terms. Not unexpectedly, the epidermis is about two to three times thicker on the hands and feet, particularly the palms and soles. The epidermis is indented by finger-like projections from the dermis known as the dermal papillae and rests on a complex junctional zone that consists of a basal lamina and a condensation of dermal connective tissue (Figure 1.3).
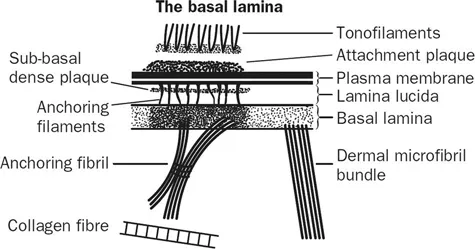
FIGURE 1.3 The junctional zone between epidermis and dermis (from Marks and Motley, Common Skin Diseases, 18E, with permission).
The cells of the epidermis are mainly keratinocytes containing keratin tonofilaments, which originate in the basal generative compartment and ascend through the Malpighian layer to the granular cell layer. The keratin tonofilaments belong to the group of subcellular structures known as intermediate filaments. They consist of polypeptides and their molecular weight ranges from 40 to 65 kD. It is thought that they provide a semi-rigid endoskeleton, and because of their connection to the desmosomal apparatus, they give strength to the epidermis as a whole. They are joined to the neighbouring keratinocytes by specialized junctions known as desmosomes. These are visible as ‘prickles’ in formalin-fixed sections but as alternating light and dark bands when viewed by transmission electron microscopy. In the granular layer, they transform from a plump oval or rectangular shape to a more flattened profile and lose their nucleus and cytoplasmic organelles. In addition, they develop basophilic granules containing a histidine-rich protein known as filaggrin and minute, lipid-containing, membrane-bound structures known as membrane-coating granules of lamellar bodies.
These alterations are part of the process of keratinization, during which the keratinocytes differentiate into tough, disc-shaped corneocytes. Other changes include a reduction in water content from 70% in the keratinocytes to 30% in the stratum corneum, and the laying down of a chemically resista...
Table of contents
- Cover
- Title Page
- Copyright Page
- Contents
- Contributors
- 1. An introduction to skin and skin disease
- 2. Signs and symptoms of skin disease
- 3. Skin infections
- 4. Infestations, insect bites, and stings
- 5. Immunologically mediated skin disorders
- 6. Blistering skin disorders
- 7. Skin disorders in AIDS, immunodeficiency, and venereal disease
- 8. Eczema (dermatitis)
- 9. Psoriasis and lichen planus
- 10. Acne, rosacea, and similar disorders
- 11. Wound healing and ulcers
- 12. Benign tumors
- 13. Malignant diseases of the skin
- 14. Skin problems in infancy and old age
- 15. Disorders of keratinization and other genodermatoses
- 16. Metabolic disorders and reticulohistiocytic proliferative disorders
- 17. Hair and nail disorders
- 18. Systemic disease and the skin
- 19. Disorders of pigmentation
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Concise Dermatology by Rashmi Sarkar in PDF and/or ePUB format, as well as other popular books in Medicine & Diseases & Allergies. We have over one million books available in our catalogue for you to explore.