Clinical Disorders of Social Cognition provides contemporary neuroscientific theories of social cognition in a wide range of conditions across the lifespan. Taking a trans-diagnostic approach to understanding these disorders, it discusses how they present in different conditions, ranging from brain injury to neurodevelopmental disorders, psychiatric conditions and dementia.
Social cognitive disorders directly impact upon individuals' work, leisure and social functioning. This book also collates and critiques the best and most useful assessment tools across the different disorders and coalesces research into intervention strategies across disorders to provide practical information about how such disorders can be assessed and treated so individuals can have meaningful, effective and satisfying social interactions.
This book is essential reading for clinicians who work with people with clinical disorders and who are looking for new knowledge to understand, assess and treat their clients with social cognitive impairment. It will also appeal to students and professionals in clinical neuropsychology, speech and language pathology and researchers who are interested in learning more about the social brain and understanding how evidence from clinical conditions can inform this.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Social cognition refers to our ability to attend to, process and interpret social signals so as to understand other people. This is the most fundamental of human abilities. As we are essentially social animals, we need to get on with others. We need to understand whether we are welcome or not, whether our behaviour is acceptable or not, whether others intend us harm or kindness. We need to be able to determine if others are interested, enthralled, bored or outraged by what we say and do, and we need to be able to modify our behaviour based on these cues so as to achieve our own social goals.
Many clinical conditions arising from developmental, psychiatric and acquired brain disorders are associated with impaired social cognition. Indeed, a systematic review of meta-analyses concluded that a wide variety of neurological disorders produced significant impairments in social cognition with moderate to large effects sizes (d = 0.41 to 1.81) that were comparable to impairments in general cognition and in some conditions, e.g. frontotemporal dementia, exceeded them. Similar, although more variable deficits, were seen in psychiatric disorders (Cotter et al., 2018). These impairments have the potential to significantly curtail psychosocial function and, therefore, are of major clinical concern. It is only relatively recently, however, that social cognition has been considered to be a cognitive domain that is distinct from non-social abilities. There are a number of sources of evidence that speak to its functional independence.
Firstly, as social animals, it is an evolutionary imperative that humans are able to interact successfully with each other. Arguably, this is more important than possessing good intellectual ability to understand the physical environment, learn and problem solve. Provided individuals are well integrated in their community, they can rely on and benefit from the group’s collective skills. This suggests that evolutionary pressures exerted on the development of social cognition are separate and possibly pre-date general cognitive abilities.
Secondly, functional neuroimaging suggests that distinct areas of the brain are activated when individuals are engaged in social compared to non-social tasks. So, for example, when thinking about oneself, thinking about psychological attributes of other people, watching emotional events or judging what kind of emotions others are experiencing, constellations of neural systems in the frontal and temporal lobes are reliably implicated.
Thirdly, there are many clinical disorders in which social and non-social abilities dissociate, that is, individuals can have profound difficulties in one realm but not the other. Autism spectrum disorders (ASD) refer to a spectrum of developmental disorders that are characterised by specific impairment in social function. Individuals with ASD can have intellectual abilities that span the normal range, including those with above average or even superior intellectual skills. Despite this, they suffer from a limited capacity to understand and interact with their social world. The converse can also be found. Williams syndrome is a rare genetic disorder that leads to profound, developmental intellectual disability. Despite this, children with Williams syndrome are highly social. They seek out the company of others and display affectionate, prosocial behaviour.
Brain damage can also selectively impair social abilities. One of the most well known cases is EVR (Eslinger & Damasio, 1985). This man was a successful businessman who underwent surgical resection of a meningioma in his frontal lobe. Following this surgery, his general intellectual abilities were assessed as intact, in the superior range. Despite this, his social abilities deteriorated, and his business eventually disintegrated. In another example, AS suffered a severe brain injury in a motor bike accident. Prior to the injury, he had been a popular member of his motorbike gang and was a well-regarded fitter and turner at the local government bus depot. Following the injury, his cognitive abilities returned to premorbid (high average) levels. However, his interpersonal skills deteriorated. He was overly talkative, egocentric and did not pick up social cues. Years after the injury, he still worked in his former position but was shunned by his work mates. He had no friends and no romantic relationships. He continued to live with his parents where he would embarrass them regularly in front of their friends with tales of buying illegal drugs and engaging sex-workers. AS participated in a number of research studies where he demonstrated that, despite good neuropsychological function, he could not understand sarcasm (McDonald, 1992) and was unable to consider the listener’s perspective when explaining a procedure (McDonald, 1993).
In dementia also, social abilities can be differentially impaired. Thus, for example, people with Alzheimer’s disease experience loss of cognitive skills such as memory and problem-solving skills early in the disease but retain social skills until the disease advances. In contrast, people who develop the behavioural variant of frontotemporal dementia show early decline of social skills, loss of emotional understanding and empathy. Meta-analytic reviews confirm that social cognitive deficits characterise people with FTD rather than AD and are independent of impairments in cognitive function (Bora, Velakoulis, & Walterfang, 2016a).
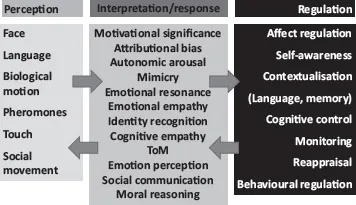
The field of social cognition is rapidly evolving and the description of its components and processes is expanding. Essentially, however, there is agreement that social cognition provides us with the ability to use social cues to represent the mental states, i.e. beliefs, feelings, experiences and intentions, of other people, as well as the ability to understand these in relation to our own mental states and to use this information to regulate our social behavior (Adolphs, 2001; Amodio & Frith, 2006). A schematic view of the stages in social cognition, i.e. perception, evaluation and regulation, is detailed in Figure 1.1.
In terms of perceptual processes, most social cognition research has been limited to the processing of visual and auditory cues (e.g. facial expressions, voice). However, it is important to appreciate that, while less studied, other sensory cues such as touch and pheromones may also play a role. Once perceptual cues have been identified, the viewer must use these and the context to infer and evaluate the mental states they represent.
In Figure 1.1, such evaluative processes include those involved in experiencing and understanding emotions as well as social cognitive ability to understand thoughts based on the behaviour and communication of others. In reality, these are probably all entwined. Finally, in order to understand others, it is critical that we are self-aware and able to understand ourselves in relation to them. We also need to be able to regulate our own reactions and emotions. For example, when we empathise, it is useful to understand how another person feels and that may involve a degree of emotional sharing or resonance. But we must also be able to step back and understand that the emotion is not ours, so as to engage in a constructive manner. Thus, we need to be self-aware, be able to differentiate between self and other, to contextualise the events that are occurring (i.e. access language, memory, executive control, etc.) and we need to be able to self-regulate our responses.
There are a number of different aspects to social cognition that have been researched extensively in clinical populations and others that are, as yet, less well delineated and understood. In the following sections, we will focus on the better-known facets of social cognition including face identity, theory of mind, emotion perception, emotional empathy, self-awareness, attributional bias, moral reasoning and social behaviour.
Figure 1.1 Processes involved in social cognition
Identity recognition
Syndromes whereby people cannot recognise the identity of other people have had a long history in neuropsychology (e.g. Bodamer, 1947) and, indeed, are among the more commonly known neuropsychological disorders in the non-scientific press thanks to popular accounts such as Oliver Sacks’ book The man who mistook his wife for a hat (Sacks, 1985). Disorders of face recognition have not typically been included in discussions of social cognition disorders with some notable exceptions (Hutchings, Palermo, Piguet, & Kumfor, 2017; Kumfor, Hazelton, De Winter, de Langavant, & Van den Stock, 2017). Being able to discriminate between strangers on the basis of face and body characteristics is fundamental to social competence and can be selectively impaired with brain lesions (De Renzi, Scotti, & Spinnler, 1969). Equally disabling is a disorder which impairs the ability to recognise the identity of familiar people, a disorder known as prosopagnosia (Bate, Bennetts, Tree, Adams, & Murray, 2019). Such face processing disorders reflect damage to the fusiform gyri, especially on the right (Watson, Huis in ‘t Veld, & de Gelder, 2016). In a particular variant of this, the patient may recognise the face but believe it is an imposter, otherwise known as Capgras syndrome. Theories regarding Capgras syndrome suggest that it arises from the normal processing of the face but a loss of attendant arousal with an associated loss of a sense of familiarity (Ellis & Young, 1990), combined with an impaired capacity to evaluate one’s own, mistaken beliefs (Coltheart, 2010). The retrosplenial cortex has been implicated in the reduction of familiarity detection in Capgras while the right ventral frontal cortex has been implicated in the impairment of the detection of expectancy violation (Darby, Laganiere, Pascual...
Table of contents
Cover
Title
Copyright
Contents
List of figures
List of boxes: case studies
List of tables
List of contributors
Acknowledgements
1 Introduction to social cognition
2 Research methodologies, brain correlates, cross-cultural perspectives
3 Impact of early brain insult on the development of social competence
4 Social cognition in autism spectrum disorder and neurogenetic syndromes
5 Disorders of social cognition in adults with acquired brain injury
6 Social cognition in psychiatric disorders
7 Social cognition in dementia syndromes
8 Social cognition in neurodegenerative diseases: Huntington’s disease, Parkinson’s disease and multiple sclerosis
9 Assessing social cognition in adults
10 Assessing social cognition in children
11 Remediating impairments in social cognition
Appendix
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Clinical Disorders of Social Cognition by Skye McDonald in PDF and/or ePUB format, as well as other popular books in Psicologia & Psicologia clinica. We have over 1.5 million books available in our catalogue for you to explore.