Marketization in the healthcare sector affects the quality and delivery of care, as well as healthcare workers' working conditions. Based on a comparison of England and Germany, along with an in-depth case study looking at New York, USA, this volume examines how trade unions respond to marketization processes and the determinants of successful strategies.
The author draws on a rich empirical study to develop a theoretical framework that accounts for sector-specific opportunity structures stemming from marketization processes and on the relevant unions' local-level leeway that opens if they build up and mobilise the available resources and capacities. The book identifies determinants of successful trade union strategies, explains the puzzling observation of similar strategic choices across different systems, and draws conclusions for prospects of trade unionism in the marketized healthcare sector. This book emphasizes the transformative effect of marketization on healthcare and the opportunities this change creates for unions, while giving special attention to the local-level conditions of trade unionism in the analysis of conflicts evolving around marketization in the hospital sector.
It is of interest to academics and practitioners working in healthcare management, human resource management, and employment relations.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
1Marketization trends and trade unions in the health sectors
1.1 Introduction
The health sector is one of the most important pillars of mature welfare states. It deals with people in their most vulnerable conditions and is therefore a particularly sensitive activity. Yet, health sectors are not organized primarily around the patients’ well-being but following economic principles, directed at cost containment and profit-making. Economic activity is widespread and ever increasing. Work in this sector is increasingly guided by economic incentives (Wehkamp and Naegler 2017). These detrimental incentives result in high costs not only for patients but also for employees in the sector. Since personnel costs clearly represent the largest share of health expenditure (Glassner, Pernicka, and Dittmar 2015, 67), they are usually the first target of cost cuts. Additionally, restructuring of work, business forms, and ownership are measures to lower costs, increase “productivity”, and profits (see, e.g., Klenk 2011). As a consequence, employees suffer from insufficient staffing and work intensification that in turn inhibits them from performing their work properly and has clearly negative effects on patients’ healthcare (see, e.g., Aiken et al. 2014). Employees in the health sector are torn between patients’ well-being, their professional ethic, and their interests as employees (Chadwick and Thompson 2000). This makes the health sector a difficult field for trade unions to organize. However, it is an increasingly important sector for trade unions to organize in: Healthcare needs are increasing, the sector is expanding, marketization is advancing, and work intensification is growing.
Trade unions are one of the few actors opposing economization of the health sector and profit-making from the ill-being of patients. They have responded with a variety of different strategies to contain marketization and ease working conditions of employees. However, their success in the past was often limited. On the one hand, they were confronted with a strong political will of economization and austerity. However, on the other hand, trade unions did not always pursue their aims with the appropriate means. They often acted regardless of the special character of the sector, its marketization trends, or local-level resources. This book provides a differentiated assessment of macro-institutional framework conditions of healthcare marketization and a detailed analysis of local-level trade union resources, capabilities, and their fit with trade union strategies. How can trade unions in the healthcare sector (successfully) respond to marketization processes, and what are the determinants of their strategies?
To answer this question, in this chapter I will first present basic information on the health sectors and marketization trends, as well as the research program. In Chapter 2, I will assess theoretical approaches to the study of trade union strategies, considering local-level resources and capabilities, as well as the sector-specific institutional framework in times of marketization. The theoretical model will then be applied to the cases studied in Chapters 3 to 6. Finally, in Chapter 7, I will connect the findings of the four empirical chapters with one another and draw more general conclusions, suggest a refined model for the study of trade union strategies against marketization in the hospital sector, and discuss the contribution and limits of this research.
In this introductory chapter, I will now proceed with the provision of basic information on marketization, the specificities of the German and English health sectors, as well as their development over the last 30 to 40 years. I will then give a brief overview of trade unions in these sectors. Finally, I will present the research design and methods of this book.
1.1.1 General marketization trends
There are two main drivers that led to the general marketization and privatization trend in healthcare across developed capitalist countries. First, driven by aging societies, technological advancements, the need for new skills and qualifications, as well as the growing power of pharmaceutical and medical equipment industries, expenditure on health was increasing at the end of the 1980s. At the same time, the gross domestic product (GDP) growth slowed down, so that taxes and social contributions decreased due to unemployment, the rise of atypical jobs, and stagnation of wages. Therefore, countries felt an increased need for austerity. Further fueled by the EU’s Stability and Growth Pact, countries started to try and contain costs also in the healthcare sector by setting incentives for competition and efficiency increases among providers (André and Hermann 2009, 130–133). This trend was intensified by the austerity measures implemented after the economic and financial crisis (Quaglio et al. 2013). The main instruments were the development of forms of privatization and marketization. In the health sector, this was done above all by means of budget setting and price controls based on the diagnosis-related groups (DRGs) (Stabile et al. 2013). Especially in the Southern European countries, this had a negative effect on health outcomes (Quaglio et al. 2013), most dramatically revealed during the Covid-19 pandemic in 2020.
Second, financial capital had become a major player and expected growing profits from the healthcare sector. Financial globalization further facilitated investment in healthcare sector assets (André and Hermann 2009, 130–133). Furthermore, private organizations were assumed to have higher efficiency, effectiveness, control of costs, and better quality (Maarse 2006, 1003).
As a consequence, the Organisation for Economic Co-operation and Development (OECD) countries have converged in healthcare regulation through the introduction of internal markets, competition, and negotiation, despite remaining differences in healthcare financing and other system-specific differences. Nevertheless, a shift from distinct types of health systems to mixed types can be observed (Rothgang et al. 2005).
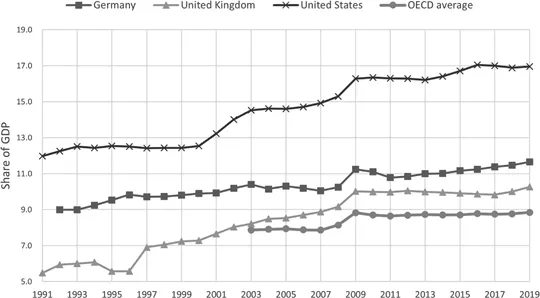
Expenditure on health shows an increasing trend in both Germany and the UK, as well as in the OECD in general. Germany started with health expenditure of 9 per cent of its GDP in 1992, and after a steep increase in 2008 and a decline during the financial and economic crisis, it grew to 11.7 per cent by 2019. The UK increased its health expenditure more than Germany, starting at 5.9 per cent of its GDP in 1991, ever increasing until 2009, then stagnating and arriving at 10.3 per cent in 2019. The OECD average (data only available from 2003) followed the same trend but was well below the German and British expenses. However, also the OECD average expenditure on health increased from 7.0 to 8.8 per cent of the GDP from 2003 to 2019 (OECD 2020c) (see Figure 1.1).
Figure 1.1Current expenditure on health, all financing schemes, and providers.
Source: (OECD 2020c).
While health expenditures increased, Rothgang et al. (2005) observed a decreasing share of public health expenditures in total health expenditure, leading to a partial shift from public to private financing. Even though total health expenditure increased, they coincided with other trends that moderate their potential positive effect on care quality, as well as on working conditions and pay for employees in the sector (see Section 1.2).
Nevertheless, it is worth noting that despite increases in health expenditures, experts nowadays agree that this cannot be referred to as a “cost explosion”. This term was frequently used in Germany in the 1990s and served as justification for the introduction of the DRG reimbursement system. The new lump-sum payments for predefined treatment procedures were to replace the full-cost compensation and were supposed to contain costs. In fact, the DRGs had the opposite effect: instead of slowing down cost increases they became a driver. The share of statutory health insurance expenditure of the GDP was stable over decades. From 1980 to 2004, health insurance expenditure was about 6.1 to 6.5 per cent. After the introduction of the DRGs it increased to 7 per cent in 2017. The increase of statutory health insurance contributions from 13.2 per cent in 1994 to 15.5 per cent in 2011 was caused by increased unemployment and low-wage increases (IAQ 2019). Also, hospital expenses of the statutory health insurance increased since 1991. However, the increase was clearly steeper after the introduction of the DRGs (Statistisches Bundesamt 2020a).
In Germany, increasing expenditure was due to a higher number of patients treated, which is expressed in increased inpatient care discharges from 23,993 per 100,000 population in 2000 to 25,478 in 2017. In the UK, this number slightly declined from 13,566 to 13,144 (OECD 2020b). Treating a higher number of patients was facilitated through a shortened length of stay in Germany. The DRGs reimbursement system set the relevant incentives. While patients in Germany stayed in hospital for an average of 16.7 days in 1990 and 11.9 days in 2000, they were released after 8.9 days in 2017. Also, in the UK, the average length of patients’ stays in hospitals decreased from 10.7 to 6.9 days between 2000 and 2017 (OECD 2020b). The increased workloads, however, were only partly compensated by an increase in healthcare employment. The number of health personnel employed in hospital (full-time equivalents) only slightly increased in both Germany and the UK during the same time period (OECD 2020a) (for more details see Section 1.2).
The mechanisms behind the described developments will be portrayed in more detail in the next sections, starting with a description of the two main concepts of privatization and marketization.
1.1.2 Defining privatization and marketization
Many of the reform trends in the two countries that will be outlined in Section 1.2 can be described with the terms privatization and marketization.
The term privatization is ideologically loaded and often used in ambiguous ways. “Privatization” is not a legal term, but an umbrella term for several forms of transfer of state tasks and responsibilities or their provision to a private legal entity. This can include a complete transfer of the task to the private sector, the provision of the task by a private provider, or the change of the provider’s legal form. German administrative science distinguishes three main types of p...
Table of contents
Cover
Half Title
Series Page
Title Page
Copyright Page
Contents
List of figures
List of tables
Acknowledgments
List of abbreviations
1 Marketization trends and trade unions in the health sectors
2 Marketization, opportunity structures, and local-level determinants of trade union action
3 Handling the beginnings of marketization: Partnership approaches to corporatization
4 Negotiating outsourcing effects: Combining partnership and organizing strategies
5 Resisting medical service privatization: Exploiting market specificities and high salience
6 Reversing marketization effects: Mobilizing workers and the public for staffing levels
7 Trade unionism in times of marketization
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Trade Union Strategies against Healthcare Marketization by Jennie Auffenberg in PDF and/or ePUB format, as well as other popular books in Business & Nonprofit Organizations & Charities. We have over 1.5 million books available in our catalogue for you to explore.