Chapter 1
Finding the health and the holistic paradigm
Action has meaning only in relationship, and without understanding relationship, action on any level will only breed conflict.
(Jiddu Krishnamurti)
Holism is not just a good idea, it’s about the way things work, the way things are. When we break things down to examine them minutely, while we become better informed about the part, we become more removed from the whole. Even complex machines ‘behave’ holistically, unlike their primitive simple counterparts, on account of their feedback mechanisms or sensors, whether mechanical or electrical; and the more sensors there are, the greater the degree of holistic function, their problems requiring a higher level of systems thinking to solve them. Now despite the holographic idea that might tempt us to believe that we might better comprehend the whole through knowledge of the part, the ‘picture’ we get of this whole diminishes in clarity as we look at these fragments in more and more detail. In other words, our relationship with the whole becomes increasingly approximate; the whole becomes less well defined as the part comes more sharply into focus.
Living organisms are a mass of sensor-based mechanisms (neural, chemical, barometric, etc.), and their health is ultimately about coherence, integration and harmony. It is about coordination, reciprocity and interconnectedness; in short, self-regulation. Furthermore, it is about the way that these properties afford the better absorption and expression of vitality (itself a phenomenon worthy of discussion a little later), so that organisms not only live ‘integrated’ within themselves, but also function with others, within a shared environment. A healthy society, for example, might not be without discord or disagreement, but it is ultimately one in which individuals share common goals or objectives or are willing to compromise respectfully to coexist. This obtains in all relationships, families, groups or organisations. The opposite situation results in unhappiness, conflict and dysfunctionality. And so it is with the body.
Dr STILL
When Still entreated us to ‘find the health’ rather than target disease per se, he might instead have suggested that we engender health, drawing it forth, by holistically engaging ill-health and impediments to its opposite. After all, we often fall into the trap of identifying disease with symptoms, instead of seeing symptoms as an expression of the body’s response to and relationship with affliction. As osteopaths we go beyond the elimination of the impediments to health, actively seeking the core of the patient’s vitality to facilitate its expression in the body, establishing its resonance throughout.
Our quest for the lack of resonance and our interpretation of it in osteopathic terms is based on:
1. the way we see ‘function’ reflected in ‘structure’, and
2. the way we appraise interplay, interaction or reciprocity of function throughout the body structure itself.
I have explored both these themes in At the Still Point of the Turning World: The Art and Philosophy of Osteopathy, in which we look at the ‘structure–function’ bonds and the concept of reciprocating tissue function.
In order to fulfil both these requirements in practice, we have to engage the potential interplay of structure and physiology coupled with the complex interplay of all tissues via neuromuscular, tensegrous and ‘energetic’ phenomena as structures affect one another in a functional way. Whereas these phenomena are naturally interwoven, we tend to break them down into component parts in order to study them. And so we speak of ‘fluidic’ elements (arterial, venous, lymphatic and CSF); neural, neuromuscular and reflex factors (somatico-visceral, viscero-somatic, somatico-somatic, somatico-psychic and psycho-somatic); ‘bio-energetic’ properties of connective tissues and the connective tissue matrix as a whole, all sustained by the piezoelectric properties of proteins (notably collagen, about 35–40% of the body’s protein) and water (99% of the body’s molecules); and the interface of connective tissue and cell function (mechanotransduction) (Lever, 2013).
When we then add to this the rhythmic oscillatory property of living tissues (Fröhlich, 1988), including that of the viscera themselves, we get closer to the fundamental preoccupation with integrated motion, mobility and motility, so central to osteopathic thinking.
To quote Fritjof Capra:
. . . living organisms are intrinsically dynamic, their visible forms being stable manifestations of underlying processes. Process and stability, however, are compatible only if the processes form rhythmic patterns – fluctuations, oscillations, waves, vibrations. Ordered structures arise from rhythmic patterns.
(Capra, 1982)
In the 16th century, philosopher Michel de Montaigne anticipated this perspective:
Tout est en perpetuelle mutation et changement (Everything is in perpetual flux and change).
HOW DOES IT WORK?
So how, in practice, do we make this happen? How do we touch in order to perceive, how do we perceive in order to interpret and how do we make those interpretations meaningful and useful in a therapeutic context? In short, how do we use ‘mind’ as well as the hands?
Well, before we answer those questions, we need to look at aspects of ‘mind’; the way our thinking interprets and contextualises our findings and our perceptions, ordering them systematically, but within a holistic approach rather than a ‘multifactorial’ one. So an initial consideration of ‘cause’ within a holistic paradigm is useful at this point.
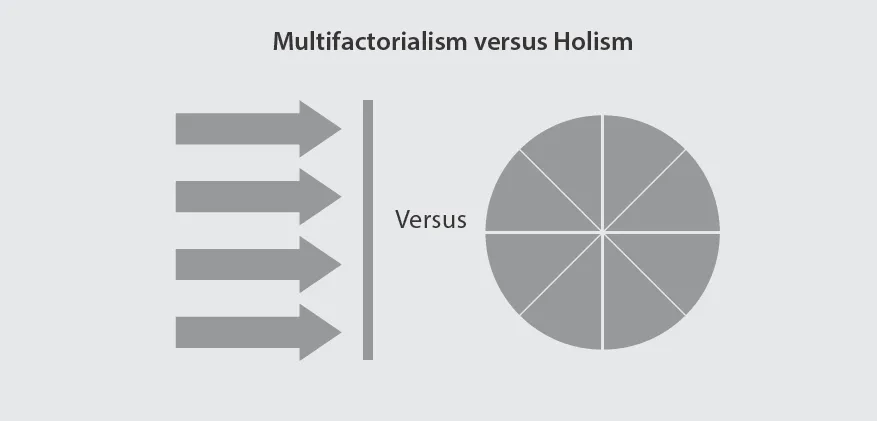
Figure 1.1
Eclectic and multifactorial approaches often involve treatments that are administered in parallel. Treatments can be conflicting and even incompatible. Holistically based treatments address the interface between multiple causes to elicit orchestrated responses that have systemic benefits.
HOLISM
Holistic causation is the simultaneous causal relationship between wholes and parts, rather than the temporal sequence of causal events.
(Tomasz Placek, 2004)
It is easy to claim to be holistic; in our modern world of ecology and globalism, the notion of interconnectedness is increasingly familiar. But the implementation of holism is a little more difficult. And so it is with osteopathic holism; not least because it involves the processing of several strands of information to create a conceptual pattern and then to determine a focal point of access, as with specific adjustment technique (SAT), or a therapeutic theme or approach when implementing other methods. Holism gives ‘shape’ or pattern to the diagnosis. (Many students, having studied all the theory and technique, still voice frustration at how an osteopathic diagnosis is made and how and where to begin once all the informational strands have been gathered.)
Origins
Although it is a term that was coined in 1926 by statesman and philosopher Jan Smuts, holism has existed as a concept since ancient times and, more recently, in the work of Spinoza, Hegel and others. Scientific holism holds that the nature and behaviour of a system can never be entirely predicted or reduced to finite component parts no matter how much is known about it; there will always be some incompleteness and uncertainty. This is reflected in quantum, complexity and chaos theories, in which despite an element of determinism, there will always be a measure of unpredictability owing to the unfathomable nature of things in the natural world. Thus, apparent randomness could be the reflection of the inevitably incomplete knowledge of all possible variables at the root of any phenomenon (as they remain concealed in what David Bohm termed ‘the implicate order’), or more accurately, their unpredictability. It would be so much easier if events and experience expressed linearity, but in reality, that isn’t the case; they express interconnectedness and probability rather than certainty.
To quote physicist Richard Feynman:
A philosopher once said, it is necessary for the very existence of science that the same conditions always produce the same results. Well, they don’t!
Furthermore, virologist and immunologist Marc van Regenmortel asserts that reductionism has reached its limit. Biological systems, he adds, ‘are extremely complex and have emergent properties that cannot be explained, or even predicted, by studying their individual parts’ (van Regenmortel, 2004).
And physicist Henry Stapp stated:
. . . the physical world is . . . not a structure built out of independently existing unanalyzable entities, but rather a web of relationships between elements whose meanings arise wholly from their relationships to the whole.
(Stapp, 1971)
Meanwhile, James Oschman’s words on this ‘quantum’ theme will be familiar to many:
The basic discovery in quantum physics is that, at the subatomic level, no particles exist except in relation to others. What we call objects are in fact points of correlation in unbroken and interconnected networks of events, motions, relations and energies – the continuum of nature.
And even more pertinently:
Subatomic particles and all matter made from them, including our cells, tissues and bodies, are patterns of activity rather than things. There is no thing that exists by itself. Living nature and the universe as a whole form a seamless dynamic web of interrelated and intercalated parts and rhythmic processes. No fundamental unit or most important part can be isolated.
(Oschman, 2000)
CAUSE
Now as a part of the process central to our work, we attempt to understand CAUSE or causal mechanisms. And within the field of natural therapeutics, we place much emphasis on ‘cause’. Some used to claim, a little arrogantly perhaps, that we treat causes, not effects, and with any given challenge, tend to think that a primary accessible cause exists – preferably in the singular – in many if not most clinical situations. However, as mathematician Franz Thomas states:
Anyone who tries to apply one-dimensional causal chains to intermeshed systems can no longer claim to be scientific.
And writer Arthur Koestler called the linear ‘cause and effect’ view of body function ‘the greatest superstition of our age – the materialistic clockwork universe of early 19th century physics’. (Koestler, 1976)
This is why the flawed interpretation and criticism (by Lederman among others) of such notions as Korr’s neural facilitation theory and its relevance to osteopathy should not be taken out of context or seen as if it were intended to be independent of the many other potential causes. Like all ‘causes’, it contributes to predisposition, not to definitive and predictable consequences in isolation.
James Marcum, Professor of philosophy and medical humanities in Texas, has investigated the growing field of systems biology, and in relation to causes states:
. . . information and entities emerge that cannot be derived or deduced from investigating just the component parts in isolation; rather, only when scientists examine the whole can they explain emergent information or properties of complex phenomena . . . In this approach, as in many but not all antireductionism approaches, causation proceeds from top to bottom or downwards. [For example] . . . carcinogenesis is the result not of lower-order perturbations, such as mutated genes, but of perturbations of higher-order entities and their properties, such as disrupted or disorganised tissues or organs.
(Marcum, 2008)
Returning to osteopathy
Many treatment approaches, including both SAT and general osteopathic treatment (GOT) can, at times, appear to be treatment models that unfold almost independently of clinical symptoms and clinical diagnosis, or of an appraisal of ‘cause and effect’, just as the cranial approach can peg itself to a format based on Sutherland’s ‘five phenomena’ or the observation of the ‘tide’. Their protocols can appear almost self-serving in that, to some extent, we treat what we find. Treatment may even become routine, whether guided by linear thinking or not. But I want to look at two contrasting points here: on the face of it, they may seem ...