eBook - ePub
Removable Prosthodontic Techniques
- 256 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Removable Prosthodontic Techniques
About this book
This manual describes the procedures required to make dentures and removable partial dentures. The book outlines each step in detail, including some clinical procedures, and emphasizes the relationship between clinical dentistry and dental laboratory technology.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
SECTION 1
Introduction to Removable Prosthodontic Techniques
The loss of permanent natural teeth is not a normal process but results from disease or accident. Tooth loss leads to changes in the face which must be understood by dentist and technician before successful replacements can be constructed.
Prosthodontics is “the branch of dental arts and science pertaining to the restoration and maintenance of oral function by the replacement of missing teeth and structures by artificial devices.” (Current Clinical Dental Terminology) The term prosthodontics is a combination of the words “prosthesis” and “dentistry” and is used synonymously with prosthetic dentistry. A prosthesis is defined as “the replacement of an absent part of the human body by an artificial part.” (CCDT) Thus, any dental restoration is a prosthesis. In common usage, however, the term prosthesis, when applied to dentistry, is used to designate an artificial replacement of a tooth or teeth and associated structures.
Prostheses are not restricted to dentistry. A prosthesis is a substitute for any natural part which has been lost. Artificial eyes and artificial limbs are both forms of prostheses, as are metallic joints or protective headplates which are implanted into the body. Prostheses have different functions. An artificial eye does not restore sight, but it does help a person’s appearance. An artificial leg does not function as well as a natural leg, but its primary purpose is to restore function. A removable dental appliance has the qualities of both an artificial leg and artificial eye in that it restores both function and appearance, but usually does not attain the efficiency or appearance of the natural part it replaces.
A denture is “an artificial substitute for missing natural teeth and adjacent structures.” (CCDT) There are many types of dentures, but we are interested primarily in two; the complete denture and the removable partial denture.
A complete denture is “a dental prosthesis that replaces all of the natural dentition and associated structures of the maxillae or mandible.” (CCDT) A partial denture is “a prosthesis that replaces one or more, but less than all, of the natural teeth and associated structures.” (CCDT) A removable partial denture is “a partial denture that can be readily placed in the mouth and removed by the wearer.” (CCDT)
It is interesting to note that in these definitions there is a reference to the teeth and associated structures. By definition, a removable prosthesis replaces more than just teeth; it also replaces bone and soft tissue which may have been destroyed by traumatic injury, by disease, or through natural processes.
The primary difference between a complete denture and a removable partial denture is the method by which the prosthesis gains support. A complete denture is supported by bone covered by soft tissue (mucosa). A removable partial denture gains support from the bone covered by mucosa, and from the remaining teeth. A removable partial denture is more stable and retentive than a complete denture due to the remaining teeth. Because of their better support, removable partial dentures are conceded by all authorities to be more efficient than complete dentures.
REVIEW OF ORAL ANATOMY
The teeth, tongue, lips, cheeks, and other oral structures with which we are concerned have several functions, among which are mastication, speech, and appearance. One cannot say that one function is more important than another. Mastication, or chewing is the first stage of digestion. Chewing is not confined to the teeth alone, but involves action of the tongue and cheeks, and all the swallowing muscles. Speech is also a function of the oral cavity. While speech is produced in the larynx, the structures in the oral cavity, along with the lips, help to make sounds intelligible.
The structures around a person’s mouth also lead to a pleasing appearance. Throughout history the mouth has been important to a person’s appearance.
A dental technician must be familiar with the structural form of the dental arches and the associated structures. Without understanding the natural structures it is difficult to recognize the changes which take place with the loss of teeth. The inclination and relationship of the anterior teeth to the lips are important factors in the restoration of normal lip contours and facial appearance. Knowledge of the natural condition is essential before the edentulous conditions can be understood. A review of the normal structures in the Dental Anatomy Manual, or a good dental anatomy text, will be worthwhile at this time.
ANATOMICAL CHANGES ASSOCIATED WITH LOSS OF TEETH
The loss of a tooth produces many changes other than just leaving a gap in the dental arch. These changes may not be apparent to the casual observer or to the indifferent patient, but an observant person will notice these changes. When a tooth is lost, the supporting bone shrinks or, in dental terminology, resorbs. Resorption is most noticeable when several teeth have been lost, and is more apparent in the mandibular arch than in the maxillary.
The face changes greatly in appearance when all the teeth are lost. The changes are due to the loss of teeth, resorption of the alveolar bone, the ability of the patient to move the mandible closer to the nose (loss of vertical dimension), and lack of support for the facial muscles. The description of the changes associated with the loss of teeth has been separated into two parts for ease of explanation.
CHANGES ASSOCIATED WITH LOSS OF MAXILLARY TEETH
The form and structure of the alveolar process of both the maxilla and mandible change when the teeth are extracted. The casual observer may think there are fewer changes in the maxillae than in the mandible after the teeth are lost. This may be true; however, the changes often are of the same magnitude in both arches, but the presence of the hard palate makes changes in the maxillae less noticeable.
Most dentists agree that the function of the alveolar processes is to provide a foundation and attachment for the teeth. When the teeth are lost, the primary function of the alveolar process is destroyed and they resorb or atrophy as does any part of the body which no longer functions (for example, muscles which are inactive decrease in size). In addition, the intraseptal portions of the alveolar process which remain after the extraction of several teeth become rounded. The combination of the elimination of sharp edges (a natural process in all organisms) and atrophy causes changes in the gross contours of the alveolar bone. The internal architecture of the bone in the alveolar processes is reoriented, becoming finer and less dense after the teeth are lost.
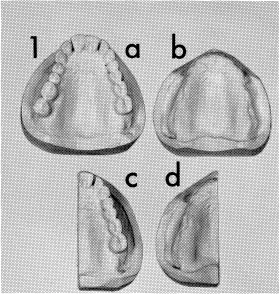
Figures 1 and 2 illustrate the bony changes which take place in the maxillae following extraction of the teeth. In Figure 1, “a” is the arch before extraction and “b” is a cast of the edentulous arch three months after extraction. Figure 1, c and d are duplicate casts which have been sectioned. The two sectioned casts have been joined in Figure 2 using anatomical landmarks in the palate to align the two halves anteroposteriorly. This is dramatic proof that bony changes occur after the extraction of the teeth. The improper placement of artificial teeth without consideration of the bony changes will result in improper support for the lips and an unnatural esthetic result.
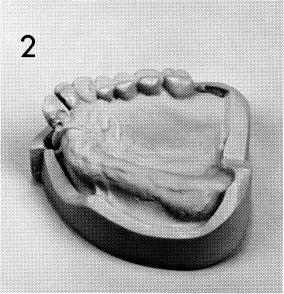
All of us have seen a horse shake his skin in one area when he is bothered by a fly. A horse can move his skin without moving another part of or any bones in his body because there are muscles in the horse’s skin. If a man has a fly on his back, he has to make a skeletal movement (move an arm or twist his body) in order to dislodge the fly. However, muscles are present in the facial region which allow a person to change his facial expression independent of any skeletal movement. We do this when we smile, frown, squint our eyes, or, in some people, wiggle our ears. The muscles of facial expression most important to the dentist and dental technician are those around the mouth (Figure 3). These muscles are supported by the teeth and the alveolar processes. The loss of teeth removes support from these muscles and without support the muscles do not function normally. If dentures do not restore lost structures and normal contours, the change around the mouth gives the individual the typical “denture look.” Proper placement of the teeth, with proper contouring of the base, will aid in eliminating this unattractive appearance.
CHANGES ASSOCIATED WITH LOSS OF MANDIBULAR TEETH
The bony changes occurring after the extraction of mandibular teeth appear greater in the mandible than in the maxillae. The resorption of the alveolar process may result in having the tissues of the cheek (buccal mucosa) more or less continuous with the floor of the mouth. Reduced area for denture support accounts for patients having more problems becoming accustomed to mandibular dentures.
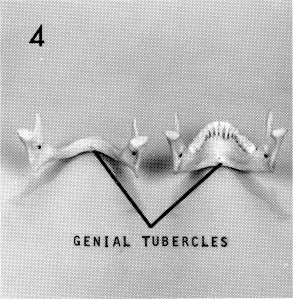
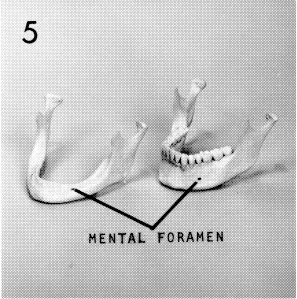
Figures 4 and 5 illustrate the changes which take place in the mandible after the teeth are extracted. It is not uncommon to find the genial tubercles at the crest of the residual ridge. When an individual has his teeth, the genial tubercles are about one and one-half inches inferior to the incisal edge of the teeth. Thus, one can see how much vertical loss of tooth and bone may occur after the mandibular teeth are lost.
The soft tissue changes which occur following the loss of teeth are different in the mandible than in the maxillae. The maxillary muscles of facial expression attach above the alveolar process. Thus the attachment or origin of these muscles remains constant, even after the maxillary teeth have been lost and the maxillary alveolar process resorbs. Proper contours may be restored to the upper lip with a denture.
The same situation does not exist in the mandible. The origin of the triangularis, mentalis and quadratus labii inferioris muscles does not remain constant after the teeth have been lost. When teeth are present these muscles attach to the facial surface of the mandible. After the teeth are lost and the alveolar process resorbs, these muscles originate on the superior surface of the mandible. In instances of severe resorption, these muscles may originate on the crest of the residual ridge.
The clinical significance of these anatomical soft tissue changes is often overlooked. Normal contours can be restored with a maxillary denture, but it is almost impossible to restore all normal contours and expression with a mandibular denture because the attachment of the muscles to the crest of the mandibular ridge changes the action of these muscles. Proper placement of the mandibular teeth helps restore normal appearance and function, but it is impossible to duplicate the original contours of the lower lip.
ANATOMICAL CHANGES AND ESTHETICS
The loss of one or more teeth affects appearance in several ways:
(a) The unattractive appearance we see when a person has lost one or more anterior teeth, the “picket fence appearance.”
(b) The change in shape of the lips or cheeks due to loss of support by the teeth.
(c) The change in a person’s appearance due to conscious or subconscious efforts to avoid smiling or otherwise showing unattractive teeth.
(d) The changes in facial contour resulting from the loss of support for the muscles of facial expression.
(e) The illusion of a prominent chin which results from the mandible being closer to the maxillae (lost vertical dimension) as a result of the loss of all the teeth in one or both arches.
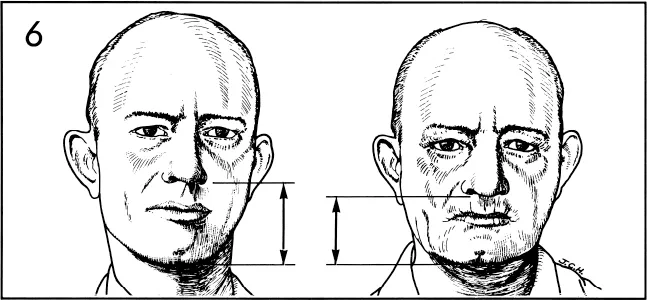
Many of the facial changes associated with the loss of the teeth are illustrated in Figure 6. The lips have lost their support with the result that the vermillion border (red portion) of the lips is thinner and creases have developed around the lips. Note the pronounced loss of support in the canine regions. The chin is closer to the nose due to a lack of vertical support which also causes the chin to be more prominent.
The degree of appearance which can be restored is dependent upon factors other than the loss of teeth and degree of resorption. The thickness of the lips and the development of the facial musculature are also factors in appearance. Men with beards and heavy lips are less likely to show the esthetic effects of severe resorption than are people who have thin musculature and tissue in the facial area. Elderly women with thin, fragile, parchment-like skin are difficult to treat with complete dentures in that it is hard to restore normal contours and good esthetics.
Proper facial contours, proper vertical dimension, and tooth selection are factors for which the dentist is responsible. It is important for a technician to understand them so that he can more intelligently follow the dentist’s prescription (work authorization) and thus work in unison with the dentist to help achieve good results.
THE TEMPOROMANDIBULAR JOINT AND JAW MOVEMENTS
The mandible articulates with the skull at the temporomandibular joints (Figure 7). The condyle of the mandible fits into the mandibular fossa on the underside of the temporal bone, thus the name temporomandibular articulation or joint.
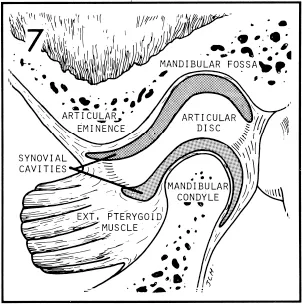
The articular tubercle or eminence is a rounded projection which forms the anterior boundary of the mandibular fossa. The articular disc is c...
Table of contents
- Fornt Cover
- Title Page
- Copyright Page
- Preface
- Contents
- 1. Introduction to Removable Prosthodontic Techniques
- 2. Preliminary Impressions and Casts
- 3. Custom Impression Trays
- 4. Master Casts
- 5. Baseplates
- 6. Occlusion Rims
- 7. Articulators, Articulator Movement, and Mounting Casts
- 8. Central Bearing Devices
- 9. Artificial Tooth Arrangement
- 10. Festooning
- 11. Flasking, Packing, Processing, and Recovery
- 12. Selective Grinding and Milling
- 13. Polishing
- 14. Clinical Remounts
- 15. Vacuum and Pressure Forming Machines
- 16. Refitting Complete Dentures
- 17. Repairs
- 18. Immediate Dentures
- 19. Single Complete Dentures
- 20. Introduction to Removable Partial Dentures
- 21. Removable Partial Denture Design
- 22. Planning, Mouth Preparation, and Final Design
- 23. Production of the Refractory Cast
- 24. Pattern Construction
- 25. Spruing, Investing, Casting, and Polishing
- 26. Corrected Impressions, Jaw Relationship Records, and Mounting Casts
- 27. Artificial Tooth Arrangement
- 28. Flasking, Processing, and Finishing Removable Partial Dentures
- 29. Removable Partial Denture Relines
- 30. Removable Partial Denture Repairs
- Index
- Back Cover
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Removable Prosthodontic Techniques by John B. Sowter, D.D.S.,John B. Sowter D.D.S., Roger E. Barton in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over one million books available in our catalogue for you to explore.