Winner of a HIGHLY COMMENDED AWARD in the Anaesthesia category of the 2010 BMA Medical Book Competition. This book comprises structured questions and answers that closely simulate the structured oral examination (SOE) format of The Royal College of Anaesthetists' final FRCA examination. The style of exam questions has changed over the years and this book matches the most recent changes in this updated exam. It consists of ten sets (chapters) of complete SOE papers. Each SOE set (chapter) includes one long case, three short cases and four different applied basic science topics (anatomy, physiology, pharmacology and clinical measurement). As this book is presented in the format of complete examination papers, it will enable candidates to assess their knowledge and skills. It will also assist trainers in setting up mock exams. With thorough revision of this book, trainees can confidently sit their exams. The authors have been organising final FRCA viva courses for the past five years, running four exam preparation courses a year, attended by about 200 trainees each year. This book includes updated knowledge based on the syllabus and more recent questions asked in the FRCA examination. It is, therefore, essential study material for trainees and a great educational tool for trainers. This book will also help candidates all over the world to pass highly competitive postgraduate examinations in anaesthesia. It is an invaluable educational resource for all anaesthetists.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineStructured oral examination 1
Clinical Anaesthesia
Long case 1
Information for the candidate
History
A 70-year-old male patient underwent elective abdominal aortic aneurysm repair 24 hours ago. His past medical history includes hypertension and ischaemic heart disease. His medications up to the day of surgery included simvastatin 30mg o.d., enalapril 10mg o.d., atenolol 50mg o.d. and aspirin 75mg o.d. He smoked 20-30 cigarettes until 6 months ago, after which he completely stopped.
The intra-operative blood loss was 1.2 litres with an aortic cross-clamp time of 65 minutes. The average urine output during the intra-operative period was 90ml/hour. Following the release of the aortic clamp, he required inotropic support for a brief period. He was transferred to the intensive care unit and ventilated overnight. Postoperative pain relief is still provided with epidural infusion of 0.125% bupivacaine and fentanyl 2μg/ml. He was weaned off the ventilator and extubated 4 hours ago.
You have been called to see the patient as he has developed shortness of breath.
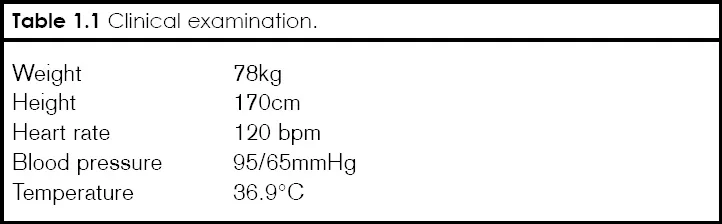
Clinical examination
He is conscious, breathless, sweaty and clammy. His peripheral oxygen saturation is 94% whilst breathing spontaneously 60% oxygen. On examining the chest there is bilateral equal air entry with crackles at both bases.
Investigations
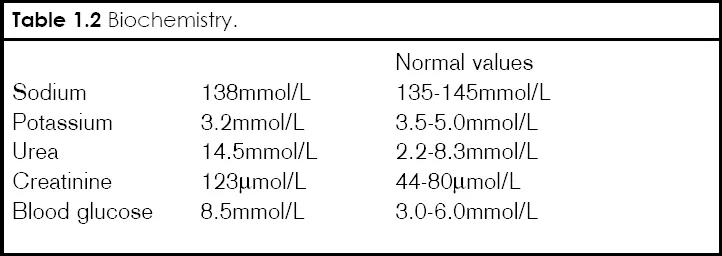
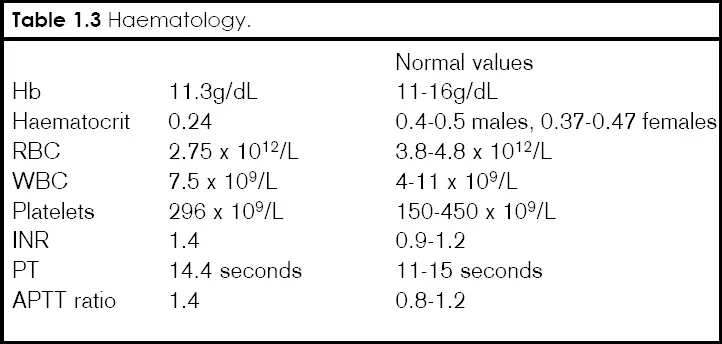

Figure 1.1 Chest X-ray.
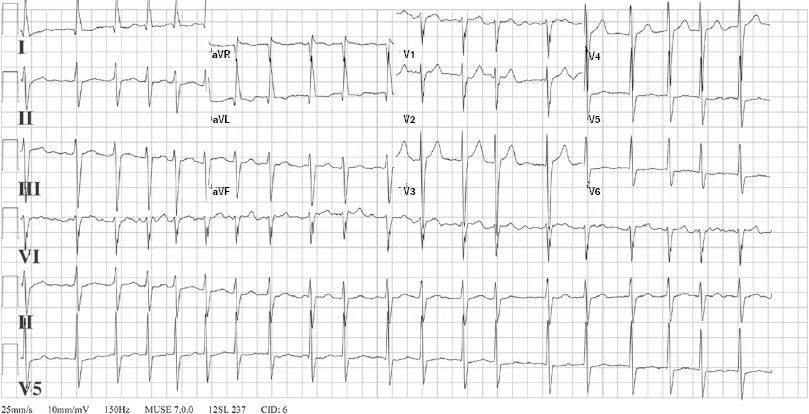
Figure 1.2 ECG.
Examiner’s questions
Please summarise the case
A 70-year-old male patient, known to have hypertension and ischaemic heart disease, recovering in intensive care following AAA repair, has developed hypotension and hypoxia at 24 hours postoperatively following tracheal extubation. His biochemistry results suggest impaired renal function and hypokalaemia.
What is the differential diagnosis?
The important causes of postoperative hypotension and hypoxia in this patient can be listed systematically as follows.
Cardiovascular system
| ♦ | Myocardial infarction. |
| ♦ | Left ventricular failure or congestive cardiac failure. |
| ♦ | Arrhythmias such as atrial fibrillation (AF). |
Respiratory system
| ♦ | Pulmonary embolism. |
| ♦ | Pleural effusion. |
| ♦ | Pneumothorax. |
| ♦ | Transfusion-related acute lung injury (TRALI). |
Metabolic causes
| ♦ | Electrolyte imbalance. |
Infection
| ♦ | Severe systemic infection (sepsis). |
Analgesia-related
| ♦ | High level of epidural blockade. |
What are the abnormal findings in the ECG?
The ECG shows atrial fibrillation as the rhythm is irregularly irregular with absent P waves and the heart rate is approximately 120 bpm. There is left ventricular hypertrophy and left axis deviation suggesting longstanding hypertension.
What are the causes of atrial fibrillation (AF)?
Cardiac causes
| ♦ | Ischaemic heart disease. |
| ♦ | Mitral valve disease. |
| ♦ | Hypertension. |
| ♦ | Cardiomyopathy. |
Non-cardiac causes
| ♦ | Hypoxia. |
| ♦ | Acute hypovolaemia. |
| ♦ | Sepsis. |
| ♦ | Electrolyte disturbances - potassium, magnesium and phosphate. |
| ♦ | Pulmonary thromboembolism. |
| ♦ | Thyrotoxicosis. |
In this patient the cause of AF is likely to be ischaemic heart disease, pneumonia and an electrolyte imbalance (low potassium).
How would you treat fast atrial fibrillation?
| ♦ | Ensure adequate airway and breathing, and administer 100% oxygen. |
| ♦ | Establish continuous ECG, blood pressure and pulse oximetry monitoring. |
| ♦ | Correct any precipitating factors where possible. |
| ♦ | Determine if the patient is stable or not. |
If the patient is unstable, he should be treated with synchronised DC cardioversion with shocks up to three attempts. If there is no response, intravenous amiodarone 300mg should be administered over 10-20 minutes and the shock repeated if needed, followed by an amiodarone 900mg IV infusion over 24 hours.
In stable patients the rate should be controlled with a beta-blocker or digoxin administered intravenously.
If the onset of AF is within 48 hours, consider amiodarone 300mg IV over 20-60 minutes followed by amiodarone 900mg ove...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Contents
- Preface
- Acknowledgements
- Abbreviations
- SOE 1
- SOE 2
- SOE 3
- SOE 4
- SOE 5
- SOE 6
- SOE 7
- SOE 8
- SOE 9
- SOE 10
- Section index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Structured Oral Examination in Clinical Anaesthesia by Mendonca, Cyprian,Hillermann, Carl,James, Josephine,Kumar, Anil in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.