The enthusiastic feedback received from readers of the international bestseller Schein's Common Sense Emergency Abdominal Surgery (now in its 3rd edition, translated to seven languages; Springer Verlag; ISBN 9783540748205) inspired the editors to do a similar book dedicated to surgical complications: practical, non-formal, internationally relevant (in all types of practice and levels of hospitals) – and definitely not politically correct: what is considered taboo by others is not taboo for us; here we discuss everything!As in the editors' previous book, the use of references is restricted to the absolute minimum, and citing figures and percentages is avoided as much as possible. The chapters in this book are the opinion of experts – each contributor has a vast personal knowledge and clinical experience in the field he is writing about. This book will help all surgeons (and their patients), avoid the misery of complications, and will provide advice on the management of those that are unavoidable. Complications and death are an integral component of surgery. Surgeons have to look death in the eyes, try to prevent it and vanquish it – this is what this book is all about."Schein's books are always terrific reads, conveying pithy observations and practical advice and doing so with wit and scholarship. This latest is surely a must for every surgeon's bookshelf." Abraham Verghese MD, author of CUTTING FOR STONE
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
What are complications? Definitions, classification and ruminations
Moshe Schein, Paul N. Rogers, Ari Leppäniemi and Danny Rosin
We have our faults and our virtues; we meet with failures and achieve successes. Many of our faults are entirely unavoidable, and arise from the fact that medicine is not an exact science… some things are quite impossible, and our work is carried out upon a living, breathing, complexity called a man, and not upon a jar, a chemical mixture in a retort, or a wooden Indian from the front of a cigar store.
J. Chalmers Da Costa
What is a complication? It is anything happening with your patient that should not have happened — any adverse event. It includes any deviation from what we know, based on our collective experience, to be the expected, uneventful intra- and postoperative course. Anything that ‘goes wrong’ is a complication!
Take for example a case of inguinal hernia repair with mesh under local anesthesia and i.v. sedation. You expect the patient to return to his room fully awake, to stand up and pee; and a few hours later to walk to the car and be driven home. After 2-3 days you want him to require no analgesia, to defecate normally and to return to his normal activities except, of course, heavy lifting and/or vigorous sports. A week later, when you see him in your office, you expect his wound to be completely healed, his scrotum pink and not swollen and his testicles soft and non-tender. Anything which deviates from the above, from normal, like wound ecchymoses or a ‘scrotal eggplant’ (aubergine) is a complication! Even something as minor as a tiny bit of pestering subcuticular suture at the edge of the incision (i.e. an aberration of healing —
Chapter 5) is a complication. “A minor complication is one that happens to somebody else!”
If we use such sensitive and all inclusive definitions of complications, and if we do search for them objectively and obsessively, and list them meticulously — almost all of our operations would be associated with complications: a strikingly high morbidity rate. Because when we cut, burn, tear, dissect, suture, staple or strangulate the human flesh, when we alter normal physiology — even for a short term — we and our patients are punished for it (
Figure 1.1).
Figure 1.1. A young doc whispers to his neighbor: “Actually, we did 25 hepatectomies in our unit — the extra zero must be a mistake. We had a few mortalities, however, just a week or so, before and after the period of the study…”
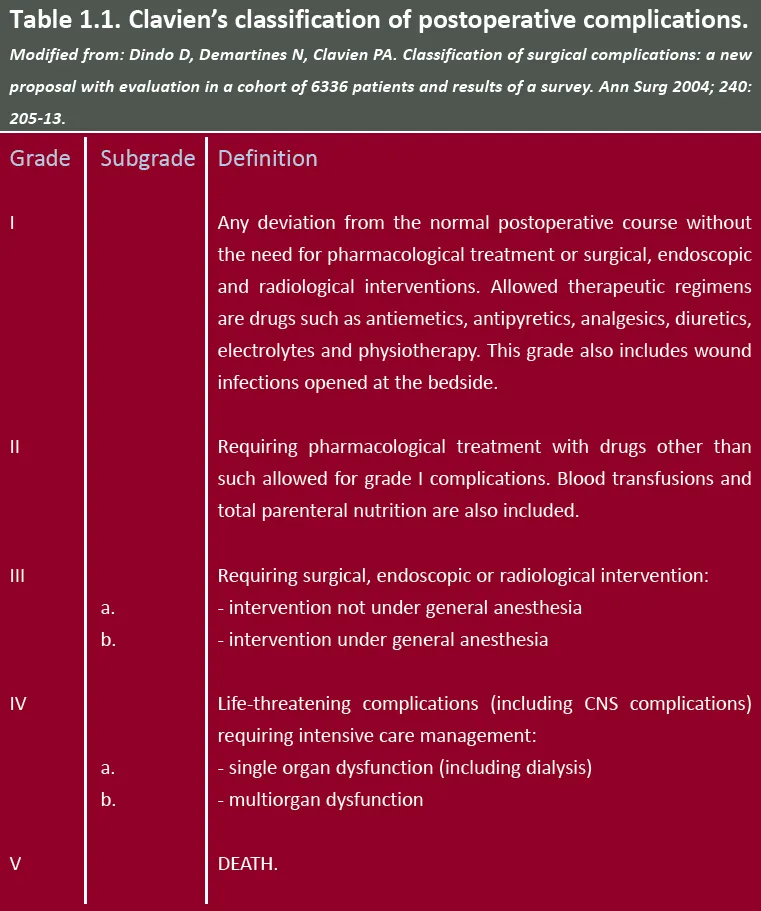
For years surgical academicians have tried to introduce elaborate classification systems of surgical complications. The classification proposed by Professor Pierre Clavien of Zurich seems to have become the most popular, having been adapted to a wide range of procedures (
Table 1.1). Other, perhaps more user-friendly systems have been suggested but none has any value in the practical management of the individual patient. They serve only as an academic or research tool: to increase uniformity in reporting outcomes, allowing comparison and analysis; they may be of value when used in departmental audits. But we, and you — not big researchers, nor technocrats — need something down to earth, more meaningful and practical.
So, in practical terms, what questions should we ask when addressing any complication?
What is the cause? Was it a result of an error of judgment or a technical mishap?
Operating on a dying terminal cancer patient indicates that your judgment has been clouded. On the other hand, having to reoperate for bleeding after a laparoscopic cholecystectomy suggests that you did not achieve adequate hemostasis of the gallbladder bed at the first operation — a technical error. Please note however that these two types of errors commonly occur in combination: the patient with ischemic intestine died because his operation was delayed (poor judgment) and his colostomy has retracted, leaking back into the abdomen (poor technique). Often, however, it is impossible to decide exactly whether a technical complication (e.g. leaking anastomosis) has been caused by poor technique (technical error) or by patient-related factors, such as poor nutrition or long-term intake of steroids.
Was it an error of commission or omission?
If you operated too late, or not at all, on a patient with necrotic bowel, it is an error of omission; but if you operated too early, or unnecessarily, it becomes an error of commission. After the operation you either failed to reoperate for the abscess (omission) or operated unnecessarily when percutaneous drainage was possible (commission). It appears that the ‘collective surgical psyche’ tends to consider errors of omission more gravely than those of commission; the latter are looked upon with sympathy: “yes, in retrospect it may have been an unnecessary operation, but at least we know now what we are dealing with…”
Was the index operation (the one responsible for the complication) indicated at all?
It is always a trade-off: what happens if I don’t operate? The graver the potential consequences of expectant management, the more acceptable it is to perform a high-risk operation, and conversely, the more minor the ailment, the higher the threshold should be for a risky operation.
“The lesser is the indication, the greater are the complications.” We do enjoy this adage but are not sure how accurate it is. What we know, however, is that a serious complication developing after an unnecessary, non-indicated, operation is a tragedy. Think about a common bile duct injury after a cholecystectomy for asymptomatic gallstones; imagine a death due to a missed bowel injury after repair of a minimally symptomatic incisional hernia in a morbidly obese patient. Some experts claim that up to a third of operative procedures performed across the world could be defined as unnecessary. The incidence of such procedures varies from country to country and place to place, depending on multiple factors — chief among the latter, we believe, are: greed (unnecessary surgery is more common where the ‘fee for service’ system exists and in locations with a higher density of surgeons) and funktionslust (in surgical terms: the pleasure of doing what one does best, or lives for — operating!). You will not find much about unnecessary surgery in textbooks. And rarely will you hear surgeons speaking about it openly. In some places, at morbidity and mortality meetings you will seldom observe anyone questioning the indication for the operation that led to the complication being discussed. So when a case of an infected aortic graft is presented, the discussion focuses on the etiology and management of this condition, but the notion that a 91-year-old patient suffering from a smallish, 5cm abdominal aortic aneurysm hadn’t needed an operation at all would be, typically, ignored. The truth is that, in many places, the subject of unwarranted, pointless, redundant surgery is still hushed — it is a taboo among surgeons and their ‘managers’. Why? Because the prevailing culture wants us to continue doing more, to earn money for the hospitals, group practices, and ourselves, to justify our existence and income. But beware — to the lawyers, advised by their surgical expert witnesses, this issue is not a taboo; and they will ask you: “Doc, why did you have to do that Nissen fundoplication? Did you try conservative treatment?” Your justification that the “patient wanted it”, that “the family pressed you to proceed” and that “an informed consent was obtained”, would not sound too convincing to the members of the jury… So think about the indication all the time and avoid redundant surgery! (
Chapter 2).
Was the complication reportable?
An increasing number of hospitals, health organizations and credentialing bodies have come up with diverse lists of reportable complications: perioperative events which, by law, have to be ‘flagged’, ‘tagged’ and reported to ‘big brother’. The rationale for such measures seems theoretically attractive: to measure the quality of hospitals and individual surgeons (weed out habitual wrongdoers) and take corrective measures, thus improving quality of care. But in daily practice such efforts do nothing more than pay lip service to popular demands. A few of the items listed as “serious reportable adverse events” do make sense ...
Table of contents
Cover Page
Title Page
Copyright Page
Contents
Contributors
Foreword
Editors’ note
Preface
Dedications
Part I — General Considerations
Part II — Specific Considerations
Epilogue: Lessons learned from surgical complications
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Schein's Common Sense Prevention and Management of Surgical Complications by Schein, Moshe,Rogers, Paul N.,Leppäniemi, Ari,Rosin, Danny, Schein, Moshe, Rogers, Paul N. , Leppäniemi, Ari , Rosin, Danny in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.