In this groundbreaking book, Charles Fishman uniquely incorporates and develops results-based accountability (RBA) into the framework of structural family therapy.
Collaborating with the founder of RBA, Mark Friedman, this approach aims to transform the field of family therapy by allowing clinicians to track performance effectively and efficiently with their clients. The book begins by reviewing the historical foundations of family therapy and evaluates why challenges in the field, alternative methods, and the reliance on evidence-based medicine (EBM) have meant that family therapy may not have flourished to the extent that many of us expected. It then explores how RBA can be integrated into intensive structural therapy (IST), with chapters examining how RBA can be applied in context, such as in treating eating disorders, supervision, and how it can be used to transform the professional's clinical contexts. Relevant and practical, the book also introduces the community resource specialist to help in the treatment of socially disadvantaged families, as well as practical appendices and "tracking tools" to empower clinicians to track their data and choose treatment models that obtain best outcomes.
This new approach offers transparent and measurable outcomes for both clinicians and training family therapists, lending a helping hand in making family therapy the gold standard in psychotherapy. It is essential reading for undergraduate and graduate students of family therapy, course leaders, and all clinicians in professional contexts, such as social workers, psychotherapists, and marriage, couple, and family therapists.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
1 The Broken Promises of Family TherapyThe Fatal Flaw
DOI: 10.4324/9781003161257-2
In the rare moments when 15-year-old Scott opened up, he confided that he has always been lonely. He was removed from his family as an infant by New Zealand social services because of his mother’s drug habit; over the years, he would return to Mom only for brief interludes. He had many caregivers in his short life. His biological dad had been in and out of prison for most of Scott’s childhood. Scott entered our residential program for severely troubled adolescents after a string of burglaries followed by a car theft and a high-speed car chase that reportedly exceeded 100 mph in a residential neighborhood.
Scott is the youngest of his mother’s six children with his father. His parents’ fractious relationship is periodically interrupted by his father’s incarcerations, as well as by their interludes with other partners with whom they also have children. Initially, Scott’s mother was reluctant to engage with our program, and when she discovered that our family therapist had contacted Scott’s father, she severed all contact. Scott’s 21-year-old brother, however, was willing to work with us.
Meeting Scott, one would be surprised by his affability, given his destructive history. He presented a tidy appearance with a welcoming smile. He was a talented artist and excelled at sports, especially rugby. He had no remorse, however, for his string of burglaries and car chases; he was cavalier regarding any possible vehicular danger to himself or innocent bystanders.
I have met many Scotts during my 16-year tenure with Windsor House. Thirty-two adolescents were residing in the one-year program when I stepped into the position. The vast majority were behaviorally identical to Scott. We had one source of referrals: the social service offices from across New Zealand. The residential setting was a former camp on many acres; previously, it had been a beautiful pastoral landscape. It was in stark contrast to the strife and poverty from which the majority of our children hailed. Our program was a brief respite from these mean streets. These adolescents were all too soon returning to their communities and anguished families. The simple goal should be to help these young people have happy, socially constructive lives.
While we and the other social agencies were the trustworthy backdrops for these children, they idealized a permanent emotional succorance from their families and, frankly, so did we. Our first order of business was family engagement. The IST model was well suited to this approach.
I advanced this model, with its foundational component of structural family therapy (SFT), which was developed in the 1960s. I was purposeful in choosing the word “intensive”; I wanted to knock on the door of complacency and urge therapists to intervene on the interactional patterns that could lead to faster change. A parent who repeatedly bails out his delinquent son, whereby the young person has no consequence to his behavior, is the homeostatic maintainer (HM) of the system and this maintains the status quo; the system is “stuck.” IST mandates that clinicians perturb the family system to reveal the HM to bring about fast change.
When I accepted my position at Windsor House, the individual psychodynamic model prevailed; family therapy was absent, nowhere to be found. Their clinical work was based on a Jungian-influenced sand tray treatment, where the therapist encouraged the client to express themselves using sand, water, and miniature objects (Sandplay Therapists of America, n.d.). These youngsters all came from embattled families in impoverished communities; the sand trays along with the one-to-one psychoanalytic therapy were “fiddling while Rome burned.” Addressing systemic change would rebuild their houses.
Sixty years ago, family therapy had so much vitality and efficacy that it looked set to take over the clinical world. It did not sit on the periphery. As I mentioned, there were two professors modernizing psychiatry during my residency training: Aaron Beck, founder of CBT, and Salvador Minuchin, founder of SFT. Beck’s model, considered innovative, was a variation of individual therapy, the prevailing paradigm of the time. He posited that behavior is modified by changing one arm of a triangle that consists of behavior, cognition, and emotions. According to Beck, changing the cognition causes changes in the other two domains and mitigates the presenting problem. This conceptualization paved the way for this widely used model of individual psychotherapy. CBT was not paradigmatically transformative. It continued to focus on the individual, as had its psychoanalytic predecessors.
By comparison, Dr. Minuchin’s model was radically new, a genuine “paradigm shift” in the tradition of T. S. Kuhn, who coined this phrase. The “patient,” according to Minuchin, was the family system. He taught us that “mind” (consciousness) is a manifestation of context; the result of an individual’s history, cognitive apparatus, and most importantly, the contemporary context that brings forth expressed tenets of the self. Treatment addresses the extracorporeal mind, that is, the influential people in a client’s social ecology. These relationships were likely maintaining the problem.
Systems theory is the theoretical foundation of family therapy (Minuchin, 1998). Gregory Bateson said that systems are like Russian dolls—“a system within a system within a system… where figures nest” (personal communication, 1979). Like the dolls, family systems are connected and nested.
A system is not just any old collection of things; it is a set of elements that are coherently organized in a way such that it achieves a goal (Meadows, 2008). Families are but one example of such a system.
In the case of drug addiction, an individual’s abuse of drugs is not seen as (only) their issue. Thus it does not matter how loving and supportive a family is toward the drug user because their good intentions will not cure the abuser. Moreover, the drug abuser with a strong desire and motivation cannot resolve their difficulties alone. The individual’s addiction can only be treated once everyone recognizes that it is a subset of a more extensive system of influences and societal issues.
(Meadows, 2008).
From our clinical family systems perspective, the family needs to do more than appreciate their involvement; members must change to “cure” the addict by restructuring their family system.
Shortly after Salvador Minuchin passed away in 2017, I published an audio blog in which I suggested that this pioneering therapist was also a brilliant scientist. He had introduced to psychotherapy the concept of “structure,” empowering clinicians to assess a family system from the observable interactions of closeness and distance against the backdrop of the developmental stages of the family members. The proximity and distance between a father and son when the boy is three years of age are very different from the closeness between them when the young man is 18. The beauty of this model, when assessing family structure, forecasts the functionality of the family.
Introduction to Psychosomatic Research
Princeton professor, T. S. Kuhn, a physicist and philosopher of science, published in 1962 the book The Structure of Scientific Revolutions. This ground-breaking book, considered a landmark in intellectual history, was where he introduced the concept of “paradigm shift,” dramatically revising how scientists view the progression of scientific theories. Previously, it was believed that the scientific method was steady, cumulative progress. Kuhn, however, saw a set of normal and revolutionary phases leading to conceptual breakthroughs that would challenge how science should work. There was a belief that scientists gathered data on which they constructed a theory; Kuhn said it was the other way around. The scientist postulated the theory, and then the scientist sought confirmation from observing and experimenting with this explanatory framework. Fifty years ago, Minuchin et al. (1978) sought confirmation of their paradigm that the locus of the problem resided in the immediate context of the family. When the child is triangulated, the child becomes symptomatic, serving a function in the family system; it diffuses the parental conflict. With the introduction of video technology, family therapists observed their videoed sessions and detected this clear pattern. When there was stress between the parents (the parental dyad), the child activated. This research, using physiological markers, confirmed the scientific theory of the family as a dynamic system/unit where the symptom stabilized the family.
Minuchin’s confirmation of his paradigm is in the form of grounded, physical findings; this approach stands out in the area of mental health, where so much flimsy theoretical substantiation is subjective responses to queries. This provided a solid foundation to develop a most effective treatment for psychosomatic conditions; moving the field of family therapy into mainstream psychiatry at the time.
Minuchin and Bernice Rosman, his collaborating psychologist, tested the validity of their psychosomatic model and published the findings in the book Psychosomatic Families (1978). Their methodology, the Family Interactional Task, generated observable scientific data. In this exercise, the family sat around a table and responded to pre-recorded queries asked by a tape player. The questions were designed to detect family interactional patterns hypothesized to maintain psychosomatic symptomatology. From this perspective, the family’s interactions, rather than the individual child, were the “patient” being assessed.
The family responded to queries such as “Discuss a recent family conflict.” While psychosomatic families struggled to answer this query, control families showed no problems in responding. Graduate students coded the videos of these sessions, blinded to the families. Their findings showed significantly different interactional patterns in the psychosomatic families. These data were reliable; these grounded interactions were spontaneous, observable responses to one another, not mediated by the researcher. This early research demonstrated that structural family therapy discovered characteristic structures.
The second part of the study, the diagnostic stress interview, was designed to determine if the psychosomatic family interactional patterns led to diabetic ketoacidosis in juvenile diabetic youngsters presenting to the Children’s Hospital of Philadelphia. Minuchin’s team postulated three discrete categories of these young people who manifested extreme lability. One group consisted of children with out-of-control diabetes because of medical factors. The second group, deemed “behavioral diabetics,” were children who deliberately manipulated their diabetic regimen for secondary gain (i.e., gorging themselves with sugar in the evening, becoming symptomatic, and thus being excused from school the next day). The third group was deemed “psychosomatic diabetics.” The families of these young people were different; they manifested certain interactional family patterns that exacerbated their children’s symptomatology. In this third group, the researchers postulated that these psychosomatic family interactions were pathognomonic for these youngsters’ out-of-control diabetes (Minuchin et al., 1978, pp. 22–29) (Figures 1.1–1.4).
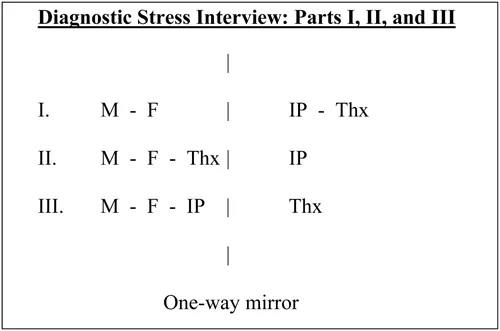
Figure 1.1 Diagrammatic presentation of the schedule of the three active periods of the diagnostic stress interview.
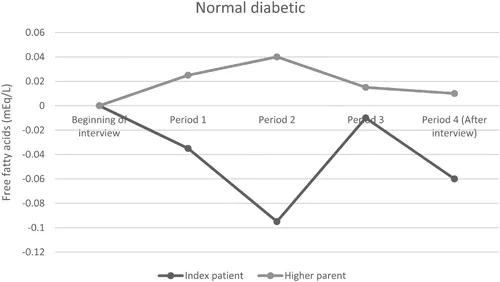
Figure 1.2 Families’ free fatty acids (FFA) during the diagnostic stress interview: “Normal diabetic” families.
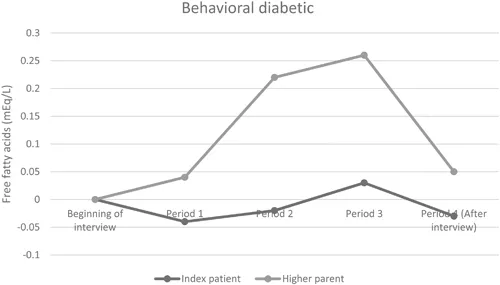
Figure 1.3 Families’ free fatty acids during the diagnostic stress interview: “Behavioral diabetic” families.
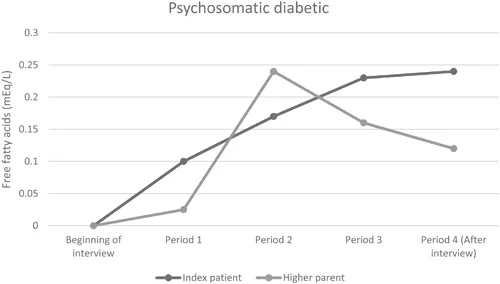
Figure 1.4 Families’ free fatty acids during the diagnostic stress interview: “Psychosomatic diabetic” families.
In part two of the study design, the child and both parents had intravenous needles through which aliquots of blood were withdrawn at regular intervals. The interview was divided into four periods. During the first two periods, the child was outside the room, observing his parents through a one-way mirror. Following a baseline discussion in which the parents spoke about neutral topics, the parents were then asked in Period I to discuss problems in the family. In Period II, the interviewer entered and exacerbated stress by siding with one parent against the other. During Period III, the child came into the room and the interviewer left. In this part, a characteristic transactional pattern is observed in psychosomatic families. The parents diffused their conflict by involving their child. As the parents’ free fatty acids fell, the child’s rose even more steeply. Period IV was a turn-off period, in which the family related alone in a room.
If one assumes that free fatty acids correlate with stress, then the triangulation can be seen as serving a function for the system. In Periods III and IV, the triangulation relieved the stress that the parents were experiencing. However, the cost to the child was demonstrated in terms of the rise of their free fatty acids and the ensuing symptomatology. This indicated the interrelationship between the child’s physiology and the family interactions, evidencing family functioning as an integrated unit.
The findings of this study supported Minuchin’s postulation of a third group, psychosomatic diabetics with specific interactional patterns. When triangulated, the diabetic child becomes ketotic, requiring hospitalization.
Dr. Lester Baker, the diabetologist involved in this research, related the following anecdote to me. The physicians at the children’s hospital called him and said they had a 12-year-old girl who was losing weight and they could find no medical cause. They asked if the PCGC psychosomatic researchers would evaluate her psychologically to see if her symptoms were psychosomatic. The family was assessed with the Family Interactional Task and did not manifest the characteristics of a psychosomatic family: there was no conflict avoidance, overprotectiveness, enmeshment, triangulation, or rigidity. Minuchin’s group called the pediatrician and reported the results: the girl was not losing weight on this psychological basis. The team suggested that the hospital would need to do further investigations. The girl was found to have a pineal tumor.
With reflection, I mused, I had come a long way from the verbal sparring in philosophy classes I experienced in college. This was scientific inquiry in front of me with observable data.
Over the decades, these basic principles of the Psychosomatic Model have been pivotal to my clinical work. For example, interactional patterns like triangulation are ubiquitous, not only in psychosomatic families but in most troubled families.
With research and scientific data, I was optimistic in the early days that the family therapy paradigm had a great future ahead of it. As a field, we were poised to make significant progress to become the mental health treatment of choice.
We are now many years from the time when the courageous founders first ventured to work with families. Family therapy certainly has made vital and significant progress, with large organizations such as the American Association of Marriage and Family Therapy (AAMFT) with 25,000 members and professional degrees such as master’s (MFT) and PhDs in family therapy. The well-known Maudsley method of family-based treatment (FBT) for working with juvenile anorexia nervosa is based on Minuchin’s model,...
Table of contents
Cover
Endorsements
Half-Title
Title
Copyright
Dedication
Contents
Preface
Acknowledgments
Introduction
1 The Broken Promises of Family Therapy: The Fatal Flaw
2 Challenging Evidence-Based Medicine: The Age of Skepticism: Studies That Define the Standard of Care Are Unreliable
3 A Case for Results-Based Accountability
4 Intensive Structural Therapy Streamlined
5 Integrating RBA and IST
6 RBA/IST for Eating Disorders
7 The Community Resource Specialist
8 Beyond Theory: Outcome-Based Supervision
9 Patterns That Connect
10 Our Challenge
Appendix
References
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Performance-Based Family Therapy by H. Charles Fishman in PDF and/or ePUB format, as well as other popular books in Psychology & Mental Health in Psychology. We have over 1.5 million books available in our catalogue for you to explore.