- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Interest in techniques to control the brain and thereby improve its function has surged, yet how realistic are these expectations and what are the ethical implications? This book reviews the main techniques of controlling brain processes for medical purposes, situating them within ethical and legal debates on autonomy and fairness.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
1
Putting the Brain in Control: From Brain Reading to Brain Communication
1.1 Locked-in
When Jean-Dominique Bauby, a successful French journalist and editor of the fashion magazine Elle, suffered a stroke in 1995 at the age of 43 his life changed completely. The stroke had affected his brainstem and when he awoke from three weeks in a coma he found himself unable to talk or move his limbs. He could only communicate through opening or closing his eyes to indicate yes or no responses. However, he was able to process information from the outside world through his sensory channels, to think, feel, evoke old memories and form new ones. We know this because, true to his profession, he went on to dictate a book, Le Scaphandre et le Papillon (The Diving Bell and the Butterfly), with the help of a speech therapist who had devised a system whereby he could form words by picking letters from visually presented streams using his eye blink responses. His book, which was also adapted into a movie, became a bestseller immediately after its release in March 1997, but Bauby died a few days after publication. Shortly before his death from pneumonia he had set up an association for those suffering from the same condition, the Association du Locked-in Syndrome.
The term locked-in syndrome describes a state when the brain is disconnected from the body and thus is locked into the skull. It can occur after lesions of the upper brainstem, the part that connects the command areas in the cerebral hemispheres with the rest of the body (except for some of the sensory channels; which explains why he could still see, hear and smell). Such lesions can be caused suddenly by a stroke or surreptitiously by motor neuron disease (MND) (also called amyotrophic lateral sclerosis (ALS)), a progressive degeneration of the motor neurons of the brain and spinal cord. Because the higher areas of the brain, the parts supporting consciousness, are generally not affected, patients are fully alert and aware of the outside world. Yet, because these higher areas of the brain are disconnected from the motor pathways that convey commands to the periphery of the body, patients have almost no control over their muscles and thus cannot walk, talk or interact with their environment in any other way, except by gaze or blink movements. These movements are only spared because their control involves nerves that leave the brain at very high levels, above those affected by the lesion, in a structure called the midbrain.
However, patients with lesions that are located even higher up in the brain may ultimately become completely paralysed and unable to engage in any way with their environment. All their movements will be reflexive and not under voluntary control. For these patients, reading questions and answers directly from their brain would be the only way to communicate. Some highly publicised efforts have evolved around the development of devices to enable the famous Cambridge physicist Professor Stephen Hawking, a longstanding MND sufferer, to communicate should he ever lose control over his facial muscles, which he is currently using to operate a computer. Although this may have sounded like science fiction just decades ago, modern brain recording techniques and fast computers now make this a real possibility.
1.2 Motor control: from brain to muscle
All our movements are produced by muscle contractions, which occur when the filaments of the two proteins actin and myosin slide against each other. The biochemical processes that result in these protein movements are triggered by the release of charged calcium particles from stores within the muscle cells. This release of calcium is triggered in turn by electrical changes in the cell that arise from its connection with a nerve at the, so-called, motor endplate (Figure 1.1). At the endplate an incoming electrical impulse is converted into a chemical signal, the release of the neurotransmitter acetylcholine, which docks onto specific receptors on the muscle cell membrane. Neurotransmitters are chemicals released by neurons that mediate the communication with other cells. Through binding to its receptor, acetylcholine opens a pore in the membrane, through which ions, small charged particles, can travel into the muscle cell and excite it electrically.
The nerve cell that connects with the muscle at the endplate commonly has its cell body in the spinal cord (Figure 1.1). Nerve cells, or neurons, have a cell body that contains the DNA (deoxyribonucleic acid), the repository of genetic information in its nucleus, and generally one main output cable, the axon, which can be several metres long in large animals. It receives its input through a system of dendrites, which can contain hundreds or even thousands of little branches. On each of these branches there can be connections (called synapses) from other neurons. A neuron can thus be connected to thousands of other neurons, which is the basis for the huge complexity of the brain. The motor nerve cell in the spinal cord, also called lower motor neuron, receives input from an upper motor neuron in the motor control area of the brain, the primary motor cortex (Figure 1.2). One important feature of the motor pathways from the brain to the spinal cord is that they cross from one side to the other – thus movements of the right arm or leg are under the control of the left motor cortex and vice versa.
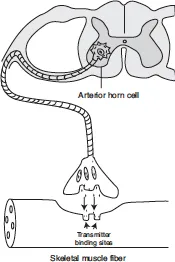
Figure 1.1 Neural control of muscle activity
Note: The axons of motor neurons in the anterior horn of the spinal connect with skeletal muscle fibres to form a motor unit. The motor neuron releases a transmitter substance that leads to changes in the electrical property of the muscle fibre and can induce it to contract. Not drawn to scale.
The initiation of a movement also involves other brain areas which are involved in motor preparation, planning and control, but a simple movement, such as the twitching of the right thumb, can be generated just by a stimulation of the appropriate area of primary motor cortex. Because the axons from upper to lower motor neurons cross over at the level of the lower brainstem, the control centre for the right hand is in the left motor cortex. And it is not even necessary to undergo brain surgery to create such a stimulation. Non-invasive devices that deliver electromagnetic impulses through the intact skull (transcranially) are powerful enough to induce such movements, even if the stimulated person tries to prevent it. This method is called Transcranial Magnetic Stimulation (TMS). Brain stimulation thus allows us to map out functional areas and if we have the option of stimulating the brain during operations directly we can obtain very detailed maps, for example the homunculus of motor representations in the primary motor cortex (Figure 1.2). This area contains the upper motor neurons responsible for movement of the whole body apart from the eyes, which have a separate motor region called the frontal eye fields, a few centimetres in front of the primary motor cortex.
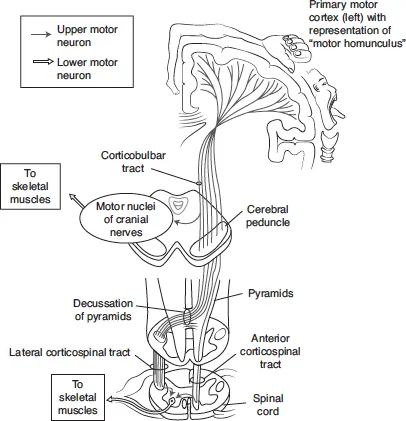
Figure 1.2 The cortico-spinal motor pathways
Note: The main motor pathway originates in the primary motor cortex of the frontal lobe of the brain, where motor neurons are arranged according to the body part to which they project (“somatotopy”, graphically depicted through the homunculus). Projections to muscles of the face and neck leave at the level of the brainstem through the motor portions of the cranial nerves. Projections to the limbs and trunk cross to the other side and travel down the spinal cord. For their further connection with skeletal muscles see Figure 1.1.
If the connections between the upper and lower motor neurons are severed, one can still form the intention to execute a movement, but the commands then cannot arrive at the appropriate muscles. If both motor tracts are cut through a lesion or otherwise destroyed (e.g. through a bleed or tumour) in the uppermost parts of the spinal cord in the neck the person will be unable to move their arms or legs. They will be tetraplegic (Greek: tetra – four; plegia – paralysis), meaning that they cannot move any of their four limbs. In these patients TMS, or even direct cortical stimulation during surgery, cannot evoke limb movements because, although the motor cortex is intact, it is no longer connected with the periphery.
If the lesion is located even higher in the brain it will, in addition, affect the pathways to the cranial nerves that control the muscles of the face and eye and thus make it impossible for the patient to articulate speech or to swallow, as in the cases of advanced MND or brainstem stroke. Only the cranial nerves that leave the brain above the level of the lesion will receive input from the motor control areas. With lesions high up in the midbrain the only nerves that are still connected to the higher motor areas may be the branches for blinking and vertical eye movements, as in the case of Jean-Dominique Bauby. The patient, or more precisely the brain, is thus almost completely locked-in, and if they go on to lose the ability to blink and move their eyes they would not have any way of expressing themselves.
How then can modern technology help locked-in patients link with the outside world? The basic idea is simple; if we can read patients’ thoughts and intentions from the intact, higher areas of their brains we might be able to communicate with them directly in the language of the brain rather than through the defective speech apparatus. The devil, though, is in the mathematical and physiological detail. At present it is not possible to read information about individual thoughts through the intact skull, and even with invasive recordings it takes many years of training for patients to convert their intentions into relatively simple motor commands (see Section 1.9). However, patients can be trained to give yes/no responses through changes in their brain activity, similar to the blinking code used by Jean-Dominique Bauby. The technique behind this simplest form of brain reading is called electroencephalography (EEG).
1.3 The electric brain
Electrical potentials in the brain can be picked up through the intact skull by EEG. The discovery and initial development of this technique was the achievement of German psychiatrist Hans Berger (1873–1941).1 Berger published his first paper on this method in 1929. What was amazing, and hitherto unknown, was the regularity of the waves of neural activity that could be picked up from the human brain during both the wake state and in sleep. The main oscillation had a frequency between 8 Hertz (Hz) and 12 Hz (8–12 peaks per second) and was called alpha rhythm by Berger. Its exact origins in the brain are still unknown but Berger knew that it must be some sort of resting or default activity of the wake brain because he could suppress it by asking his subjects to engage in effortful mental activity, for example mental arithmetic. Such manipulation brought about faster, smaller waves, which he called beta rhythm. Conversely, when subjects dozed off their EEG became slower. Heated debates on the functional significance of EEG rhythms arose immediately after Berger published his findings, for example between him and the leading British neurophysiologist Edgar (later Lord) Adrian, 1932 Nobel laureate. Adrian and his colleague Bryan Matthews conducted a series of experiments which ruled out that the EEG rhythms were artefacts arising outside the brain, for example from eye movement, supporting Berger’s view that the EEG reflected nerve activity in the brain. Yet they also contradicted Berger’s view that the alpha rhythm, called Berger rhythm by Adrian in honour of its discoverer, was generated throughout the brain and tried to localise its origin in the occipital areas at the back of the brain, the site of the visual cortex. Because opening the eyes suppresses the Berger rhythm (Figure 1.3), in the same way as effortful mental activity did, they concluded that this rhythm represented the synchronous oscillation of the visual cortex at rest, which was disrupted by visual stimulation.2
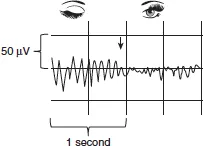
Figure 1.3 EEG trace with eyes closed (showing the alpha, or Berger, rhythm) and opened (showing the suppression of the rhythm)
Adrian and Matthews also conducted the first neurofeedback experiment (although they did not use this term), whereby they converted the amplitude of EEG activity into sound signals and monitored the EEG changes produced by opening and closing the eyes:
Again some of the evidence on the effect of opening the eyes in the dark was made by one of us listening to the rhythm from his head in a loud speaker. This made it possible to correlate the impression of not looking or looking with the presence or absence of the rhythm. In this case, as when the eyes are opened in daylight, the subject can hear that the rhythm ceases.2
Over many decades EEG was the main tool for registering brain activity non-invasively in humans. Because EEG has a very high temporal resolution and can track the activation of neural networks at a millisecond scale researchers developed techniques that allowed them to couple EEG recordings with the presentation of specific stimuli and then trace the sequence of activation across the brain. Such evoked potential studies have been conducted with all types of sensory stimulus. For example, after the presentation of a picture one can record the first evoked potential over the visual cortex after 70 ms–100 ms, followed by waves that correspond to specific stimulus properties or to the cognitive task of the participant. One particularly well-studied brain wave is the P300, a positive wave starting about 300 ms after the presentation of a stimulus, which indexes attention and working memory (Figure 1.4). It is most strongly evoked by, so-called, oddball protocols, where a regular sequence of stimuli is disrupted by a rare stimulus, the oddball. For example if rare high tones are interspersed in sequences of low tones, the high tones will evoke a P300. Conversely, if the low tones are rare and the high tones common, the low tones will evoke the P300. This wave can even be evoked by the omission of an expected stimulus. It thus indexes expectancy, which is the product of attention and memory, rather than any specific attributes of the stimulus. In fact, it can be evoked in relatively similar fashion by pictures, sounds or tactile stimuli.
The P300 therefore allows researchers to gain some insight into the mental state of a person, for example by determining whether a particular stimulus was expected or not. This wave is of interest for brain communication devices because, to some extent, it is under voluntary control. If a locked-in patient can be trained to produce a P300 whenever he or she sees the letter that comes next in the word that they are trying to form, even patients without the capacity to move their eyes or blink could ultimately dictate letters, or even books like Jean-Dominique Bauby. We will see that such a P300 speller is indeed one of the potential brain computer interfaces being developed for brain communication with paralysed patients.
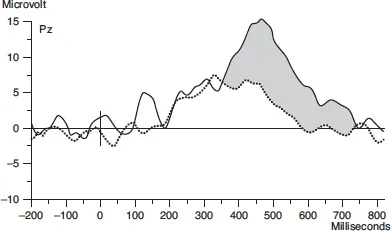
Figure 1.4 Example of the P300 wave evoked by rare stimuli (filled line), but not frequent stimuli (dotted line) in a visual oddball paradigm
Note: The EEG trace was recorded at electrode Pz, which describes a location centrally above the parietal lobe. Adapted from Linden, Prvulovic, Formisano, Völlinger, Zanella, Goebel and Dierks 19993 with kind permission of Oxford University Press.
Another important way of categorising EEG activity uses the main frequency of its oscillatory rhythm. The frequency bands below Berger’s alpha rhythm (8 Hz–12 Hz) are called theta (3.5 Hz–8 Hz) and delta (below 3.5 Hz) bands. They are dominant during deep sleep. Conversely, during cognitive activation the EEG can go into higher frequency oscillations, in the beta (12 Hz–30 Hz) or gamma (30 Hz–100 Hz) bands,4 although the higher range of this activity is of low intensity and can only be extracted by computer analysis rather than be appreciated with the naked eye (Figure 1.5). Such computer analysis of the frequency spectrum can also be used to feed the relative strength of these frequency bands back to a person in real-time and train them to change this pattern through neurofeedback (NF). One example is the study of young musicians who were trained to increase their theta rhythm to improve performance (see Section 3.2).
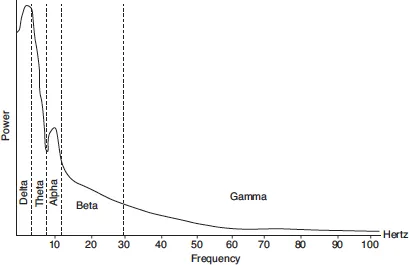
Figure 1.5 The frequency bands of the EEG
Note: The contribution of different frequency bands to the EEG at rest. The contribution to the overall electrical activity is inversely related to the frequency, with the exception of a peak in the alpha range. Cognitive activity can be associated with further peaks in the higher (beta, gamma) frequency ranges.
1.4 The biggest network in the universe
Even a high resolution EEG cap with 256 electrodes only captures the complexity of the brain in very crude ways. The human brain contains about 80 billion (1 billion = 1,000,000,000) neurons, more than the estimated number of stars in the universe. About 20% of the neurons are located in the cerebral hemispheres, forming a 2 mm–4 mm thick sheet called the cerebral cortex. The cerebral hemispheres are conventionally divided into f...
Table of contents
- Cover
- Title
- Introduction
- 1 Putting the Brain in Control: From Brain Reading to Brain Communication
- 2 External Control of the Brain: Brain Stimulation and Psychiatric Surgery
- 3 The Brain Controls Itself: From Brain Reading to Brain Modulation via Neurofeedback
- 4 The Ethics and Politics of Brain Control
- Glossary
- References
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Brain Control by D. Linden in PDF and/or ePUB format, as well as other popular books in Psychology & Neurology. We have over one million books available in our catalogue for you to explore.