eBook - ePub
International Nutrition: Achieving Millennium Goals and Beyond
78th Nestlé Nutrition Institute Workshop, Muscat, March 2013
- 181 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
International Nutrition: Achieving Millennium Goals and Beyond
78th Nestlé Nutrition Institute Workshop, Muscat, March 2013
About this book
The UN Millennium Development Goals (MDG) in nutrition are at the core of this book, with special attention to young women and their children. The first part is dedicated to the overall analysis of the world nutrition situation as related to achieving the MDG. The chapters cover the global distribution of malnutrition and micronutrient deficiencies in young women and infants, and the disease burden related to it. The second part reviews the measures taken to achieve the MDG and the potential contributions of nutrition-specific and disease control interventions (particularly with regard to reducing child and maternal mortality), as well as the possible role of sectors other than health. The last part looks into the future, scrutinizing the causes and consequences of non-communicable disease in both the developing and developed world, as well as reviewing the latest scientific evidence for underlying mechanisms and discussing the implications for public health and policy makers.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Pediatric MedicineEvidence on Interventions and Field Experiences
Black RE, Singhal A, Uauy R (eds): International Nutrition: Achieving Millennium Goals and Beyond.
Nestlé Nutr Inst Workshop Ser, vol 78, pp 59-69, (DOI: 10.1159/000354941)
Nestec Ltd., Vevey/S. Karger AG., Basel, © 2014
Nestlé Nutr Inst Workshop Ser, vol 78, pp 59-69, (DOI: 10.1159/000354941)
Nestec Ltd., Vevey/S. Karger AG., Basel, © 2014
______________________
Interventions to Address Maternal and Childhood Undernutrition: Current Evidence
Zulfiqar A. Bhutta · Jai K. Das
Division of Women and Child Health, The Aga Khan University, Karachi, Pakistan
______________________
Abstract
The global burden of undernutrition remains high with little evidence of change in many countries. We reviewed the evidence of the potential nutritional interventions and estimated their effect on nutrition-related outcomes of women and children. Among the maternal interventions, daily iron supplementation results in a 69% reduction in incidence of anemia, 20% in incidence of low birthweight (LBW) and improves mean birth-weight. MMN supplementation during pregnancy has been shown to significantly decrease the number of LBW infants by 14% and small for gestational age (SGA) by 13%. Balanced protein-energy supplementation reduces the incidence of SGA by 32% and risk of stillbirths by 38%. Antimalarials when given to pregnant women increase the mean birthweight significantly and were associated with a 43% reduction in LBW and severe antenatal anemia by 38%. Among the neonatal and child interventions, educational/counseling interventions increased exclusive breastfeeding by 43% at 4-6 weeks and 137% at 6 months. Vitamin A supplementation (VAS) reduces all-cause mortality by 24% and results in a 14% reduction in the risk of infant mortality at 6 months. Intermittent iron supplementation in children reduces the risk of anemia by 49% and iron deficiency by 76%, and significantly improves hemoglobin and ferritin concentration. Preventive zinc supplementation in populations at risk of zinc deficiency decreases morbidity from childhood diarrhea and acute lower respiratory infections, and increases linear growth and weight gain among infants and young children. Among the supportive interventions, hand washing with soap significantly reduces diarrhea morbidity by 48%, though it depends on access to water. The effect of water treatment on diarrhea morbidity also appears similarly large with a 17% reduction. Recent research has established linkages of preconception interventions with improved maternal, perinatal and neonatal health outcomes, and it has been suggested that several proven interventions recommended during pregnancy may be even more effective if implemented before conception. These proven interventions, if scaled up have the potential to reduce the global burden of undernutrition Substantially.
© 2014 Nestec Ltd., Vevey/S. Karger AG, Basel
Introduction
The State of Food Insecurity estimates that around 870 million people globally have been undernourished (in terms of dietary energy supply) in the period 2010-2012 [1]. The vast majority of these, 852 million, live in developing countries, where the prevalence of undernourishment is around 14.9% [1]. Though many countries are on track in reducing income poverty [Millennium Developmental Goal (MDG) la], less than a quarter of developing countries are on track to achieve the goal, of halving undernutrition (MDG 1c) by the year 2015. The global burden of undernutrition remains high with little evidence of change in many countries despite economic growth, and still millions of people are faced with starvation and malnutrition, with women and children contributing the major share. The progress has also been hampered by the global increase in food and oil prices, climate change, unprecedented draughts and increased number of countries affected by fragility, conflict and emergencies. According to the World Bank, 33 countries fall in the fragile situations category and, in addition, conflict and fragility also occur at the subnational level within some strongly performing countries. The World Bank further estimated that the food price crisis in 2008 pushed as many as 130-155 million more people globally into extreme poverty with an increase in the number of children suffering permanent cognitive and physical injury due to malnutrition by 44 million.
Malnutrition, including micronutrient deficiencies, remains one of the major public health challenges, particularly in developing countries [2]. Poor maternal nutrition contributes to at least 20% of maternal deaths, and increases the probability of other poor pregnancy outcomes including newborn deaths [2]. Low body mass index among women of reproductive age is an important risk factor for intrauterine growth restriction, low birthweight (LBW) and neonatal mortality. Other maternal indicators for poor pregnancy and neonatal outcomes include low maternal stature, anemia and other micronutrient deficiencies.
In the year 2011, almost 6.9 million children under 5 years of age died worldwide [3], and undernutrition was an underlying cause in about one third of these deaths which included stunting, severe wasting, deficiencies of vitamin A and zinc, and suboptimal breastfeeding. Globally, around 165 million children under 5 suffer from stunting, 101 million are underweight and 52 million are wasted, and approximately 90% of these live in just 36 countries with the highest prevalence in Southeast Asia and Sub-Saharan Africa [4] (fig. 1). Prevalence of malnourished children has decreased, and progress has been made in the past two decades, but at the current rate of progress, United Nations regional goals are unlikely to be met in all developing countries, and micronutrient deficiencies remain widespread among women and children globally.
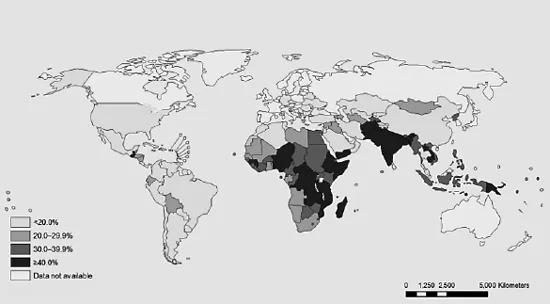
Fig. 1. Latest country prevalence estimates for stunting among children under 5 years of age. Source: http://www.who.int/nutgrowthdb/jme_unicef_who_wb.pdf.
To address this persistent burden of undernutrition in women and children and to the population at large, various strategies have been employed worldwide. Among these are nutrition education, dietary modification, food provision/supplementation, agricultural interventions including bio-fortification, micronutrient supplementation and fortification. Apart from these direct nutritional interventions, programs to tackle the underlying causes of undernutrition including prevention and management of infections (like diarrhea and malaria) have also been initiated and implemented at various levels of care. Parallel programs have also been pursued to increase coverage and aid uptake of these primary interventions including provision of financial incentives at various levels, home gardening and community-based nutrition education and mobilization programs. Although all these strategies have shown success and proved to be effective, a coherent, multifaceted and integrated action which has the global consensus is lacking, and several attempts at developing consensus is fraught with controversies and lack of coordination between various academic groups and development agencies.
Concerns for these deprived prospects have called for improved efforts to speed up and scale up the implementation of effective interventions in a systematic manner to achieve high and equitable coverage of interventions. In the following sections, we will review various interventions (table 1) and their evidence-based proven effectiveness.
Review of Interventions
Micronutrient Supplementation
The World Health Organization (WHO) estimates that in spite of recent efforts in the prevention and control of micronutrient deficiencies, over two billion people are at risk for vitamin A, iodine, and/or iron deficiency globally [5]. Other micronutrient deficiencies of public health concern include zinc, folate, and the B vitamins. In many settings, more than one micronutrient deficiency coexists, suggesting the need for simple approaches that evaluate and address multiple micronutrient (MMN) malnutrition [6]. Micronutrient supplementation is the most widely practiced intervention to prevent and manage single or MMN deficiencies. Various programs are in place to address these micronutrient deficiencies through supplementation, and evidence from evidence-based systematic reviews suggests that among pregnant women, daily iron supplementation is associated with a 69% reduction in incidence of anemia at term, 66% reduction in iron deficiency anemia at term, 20% reduction in incidence of LBW and improved birthweight [7]. Calcium supplementation during pregnancy is associated with a 52% reduction in the incidence of preeclampsia and 24% reduction in preterm birth with an increase in birthweight of 85 g, while no significant impacts were observed on perinatal mortality [8]. MMN supplementation during pregnancy significantly reduces the incidence of LBW infants by 11% and small for gestational age (SGA) by 13%. When compared with iron and folate supplementation while the impact on preterm birth, miscarriage, preeclampsia, maternal mortality, perinatal mortality, stillbirth and neonatal mortality was statistically not different [9]. Evidence of micronutrient supplementation in children indicates that vitamin A supplementation (VAS) reduces all-cause mortality and diarrhea-specific mortality by 24% and 28%, respectively [10]. VAS also reduces the incidence of diarrhea by 15% and measles morbidity by 50%; however, there was no significant effect on the incidence of respiratory disease. Iron supplementation in children results in a 49% lower risk of anemia and a 74% lower risk of iron deficiency with higher serum hemoglobin and ferritin concentration, while nonsignificant impacts were observed for height-for-age and weight-for-age [11]. Zinc supplementation at a dose of 10 mg zinc/day for 24 weeks could lead to a net gain in height of 0.37 cm (±0.25) [12] and reduce the incidence of diarrhea by 13% and pneumonia morbidity by 19%, while has nonsignificant effects on mortality [13]. MMN supplementation with 3 or more micronutrients in children showed small effect sizes for length/height and weight, with limited evidence for an impact on outcomes such as morbidity and cognitive function [14].
Table 1. Interventions to improve maternal and child undernutrition and estimates
Intervention | Estimates |
Maternal interventions | |
Iron/iron-folate supplementation | LBW (RR: 0.80, 95% CI: 0.68-0.97), birthweight (mean difference, MD: 30.81 g, 95% CI: 5.94-55.68), serum hemoglobin concentration at term (MD: 8.88 g/l, 95% CI: 6.96-10.80), anemia at term (RR: 0.31, 95% CI: 0.19-0.46), iron deficiency (RR: 0.43, 95% CI: 0.27-0.66), iron deficiency anemia (RR: 0.34, 95% CI: 0.16-0.69), side effects (RR: 2.36, 95% CI: 0.96-5.82), while nonsignificant impacts on premature delivery, neonatal death, congenital anomalies. |
Maternal calcium supplementation | 52% reduction in the incidence of preeclampsia (RR: 0.48,... |
Table of contents
- Cover Page
- Front Matter
- World Nutrition Situation
- Evidence on Interventions and Field Experiences
- Future Perspectives: Impact of Early Life Nutrition
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access International Nutrition: Achieving Millennium Goals and Beyond by R. E. Black,A. Singhal,R. Uauy,R.E., Black,A., Singhal,R., Uauy, R. E. Black, A. Singhal, R. Uauy in PDF and/or ePUB format, as well as other popular books in Medicine & Pediatric Medicine. We have over 1.5 million books available in our catalogue for you to explore.