eBook - ePub
Ocular Tumors
- 112 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Rapid advances in the field of oncology have made the diagnosis and treatment of intraocular tumors more and more complex, therefore requiring equally advanced training and expertise. Early detection and specialized care can have a profound impact on the final outcome, so it is crucial to manage them appropriately. In this 7th volume of the 'ESASO Course Series', the focus is on ocular tumors, including diagnosis and management. With a strong emphasis on diagnostic aspects, chapters cover and illustrate a variety of intraocular tumors, such as retinoblastoma and uveal melanoma, encountered in children and adults. This book includes contributions by renowned experts from Europe and the United States. It is a valuable resource for primary care ophthalmologists as well as residents and fellows in the field of ophthalmology.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
Singh AD, Seregard S (eds): Ocular Tumors.
ESASO Course Series. Basel, Karger, 2016, vol 7, pp 28-44 (DOI: 10.1159/000444380)
ESASO Course Series. Basel, Karger, 2016, vol 7, pp 28-44 (DOI: 10.1159/000444380)
______________________
Intraocular Vascular Tumors
Aleksandra Petrovic · Leonidas Zografos · Ann Schalenbourg
Department of Ophthalmology, University of Lausanne, Jules-Gonin Eye Hospital, FAA, Lausanne, Switzerland
______________________
Abstract
Intraocular vascular tumors are rare and are often associated with various ophthalmic or systemic anomalies. Choroidal vascular tumors encompass circumscribed and diffuse choroidal hemangiomas, with the latter presenting as part of Sturge-Weber or Klippel-Trenaunay syndrome. Primary vascular tumors of the retina include sporadic retinal hemangioblastoma or capillary hemangioma(s) associated with von Hippel-Lindau's disease, retinal cavernous hemangioma that is isolated or associated with Gass' syndrome, and arterio-venous malformations as part of Wyburn-Mason syndrome. Retinal vasoproliferative tumors are now considered as reactive retinal astrocytic tumors rather than true hemangiomas.
© 2016 S. Karger AG, Basel
Intraocular vascular tumors can lead to severe or complete loss of vision due to exudation, hemorrhage and serous retinal detachment. Treatment is indicated for the majority of lesions and aims to maintain or restore visual function. The choice of therapeutic approach depends mainly on the type, size and location of the tumor as well as the extent of the serous retinal detachment.
Choroidal Vascular Tumors
Choroidal vascular tumors include circumscribed and diffuse choroidal hemangiomas. These are rare, benign tumors whose incidence is estimated at about 0.02/ 100,000 new cases per year [1].
Circumscribed Choroidal Hemangioma
Circumscribed choroidal hemangioma is considered as a hamartoma without any associated local or systemic disorders. It is more common in males and has a mean age at diagnosis between 40 and 60 years [1, 2].
Clinical Presentation
Circumscribed choroidal hemangioma is often asymptomatic unless it involves the fovea, producing a slowly progressive hyperopia. Chronic secondary pigment epithelial changes at the surface of the tumor, including pigment epithelial hyperplasia and fibrous or osseous metaplasia, can cause permanent visual loss if located in the macular area. Circumscribed choroidal hemangioma is usually diagnosed once complications, such as cystoid macular edema or a serous retinal detachment, result in symptoms, such as reduced visual acuity, metamorphopsia, micropsia or flashes of light.
On fundus examination, circumscribed choroidal hemangioma appears as a red-orange choroidal mass with margins that are sometimes surrounded by a pigmented ring consisting of compressed uveal melanocytes (fig. 1a, 2a) [1, 2]. These tumors are mainly located posterior to the equator. Circumscribed choroidal hemangioma can be overlooked during a routine eye examination and may remain clinically stable or show enlargement and progressive intra- and/or subretinal exudation. As a result, cystoid edema can develop on the tumor surface, with the cysts sometimes coalescing, leading to retinoschisis. Symptomatic circumscribed choroidal hemangiomas are often surrounded by a serous retinal detachment. Optical coherence tomography (OCT) is particularly helpful in evaluating these secondary retinal changes (fig. 3).
On B-scan ultrasonography, a dome-shaped choroidal mass is observed (fig. 4a), while the internal reflectivity of the tumor on A-scan ultrasonography is characteristically high (>80%) because of its density, reflecting its intrinsic vessels’ walls (fig. 4b). Differential diagnosis includes equally red-orange, highly reflective carcinoid or clear renal cell choroidal metastases, especially when these present as a single lesion.
Fluorescein angiography (FA) has limited value in the diagnostic approach. Meanwhile, in some cases, FA can reveal a so far unnoticed choroidal hemangioma, appearing as a nonspecific hyperfluorescent mass with a fine, lacy intrinsic vascular network.
Indocyanine green (ICG) angiography in choroidal hemangiomas is pathognomic. During the arterial phase, strong hyperfluorescent vessels appear within the masking tumor mass (fig. 1b, 2b), which, during the venous phase, becomes increasingly hyperfluorescent (fig. 1c, 2c). In the late phases, the tumor is hypofluorescent compared to the surrounding choroid, referred to as a ‘washout’ phenomenon and related to accelerated dye outflow from the hemangioma (fig. 1d, 2d) [3].
Histopathology
Currently, as the diagnosis of circumscribed choroidal hemangioma can be confidently made based on its clinical presentation, the indication for a diagnostic biopsy should be an exception. In 1975, Witschel and Font [4] studied 71 choroidal hemangioma specimens, including 45 circumscribed and 17 diffuse choroidal hemangiomas. They distinguished capillary, cavernous and mixed-type hemangiomas, all consisting of vascular channels lined by endothelial cells without any mitoses.
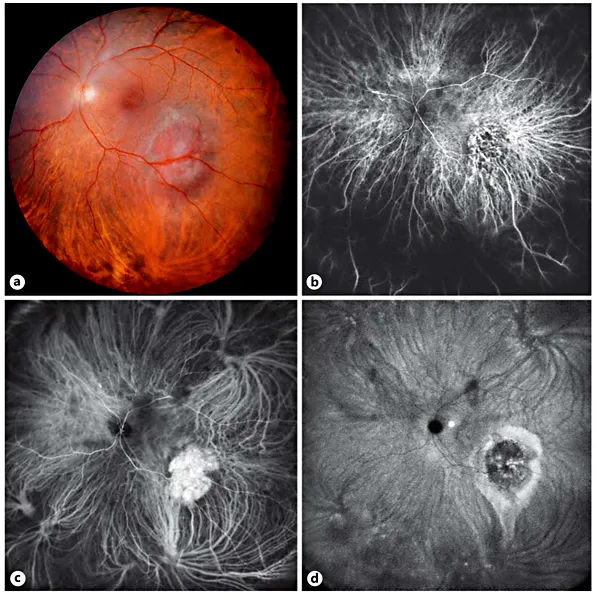
Fig. 1. Small circumscribed choroidal hemangioma. a Panoramic color fundus picture. Temporal, inferiorly located dark red tumor with pigmented margins. b Panoramic ICG angiography: arterial phase. Prominent intralesional, dilated vessels. c Panoramic ICG angiography: venous phase. The entire tumor is filled with contrast dye. d Panoramic ICG angiography: late phase. The tumor, being ‘washed out’, is surrounded by a hyperfluorescent area associated with a gravitational epitheliopathy.
Management
Circumscribed choroidal hemangiomas are benign tumors, and treatment should aim at maintaining or restoring vision. Small, nonevolutive hemangiomas without serous retinal detachment of the macula or significant pigment epithelial alterations are usually observed periodically.
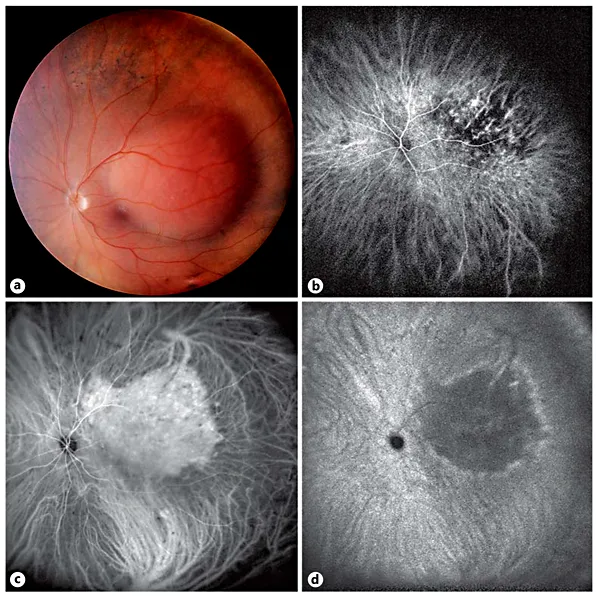
Fig. 2. Large circumscribed choroidal hemangioma. a Panoramic color fundus picture. Large red-orange tumor that is temporal and superiorly located and in contact with the fovea. b Panoramic ICG angiography: arterial phase. Intralesional, dilated vessels. c Panoramic ICG angiography: venous phase. The contrast dye fills the tumor, whose margins appear slightly more spread out compared to the ophthalmoscopic image. d Panoramic ICG angiography: late phase. The tumor presents a ‘washout’ phenomenon and is surrounded by a hyperfluorescent area.
Currently, the most used therapeutic techniques are photodynamic therapy (PDT) and radiation therapy. PDT, a routine treatment for age-related macular degeneration before the availability of intravitreal anti-vascular endothelial growth factor injections, consists of intravenously injecting a photosensitizer, followed by applying a 689 nm laser [5] to the entire tumor surface, whose contours are best defined on ICG images of the venous phase. The stimulation of this photosensitizer by nonthermal red light produces reactive oxygen radicals, damaging the endothelium, with subsequent occlusion of the vascular channels, tumor atrophy, subretinal fluid resorption and retinal sparing. PDT is most effective in relatively small, nonrecurring choroidal hemangiomas that do not present major pigment epithelial alterations (fig. 5). PDT is relatively cheap and accessible, but recurrence of the serous retinal detachment is possible, and retreatment can lead to choroidal or retinal atrophy, producing additional loss of vision.
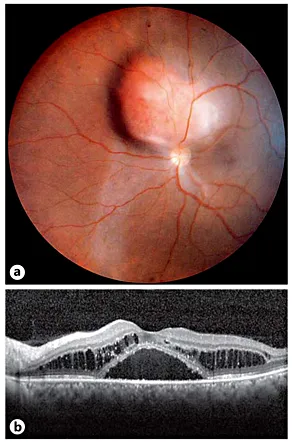
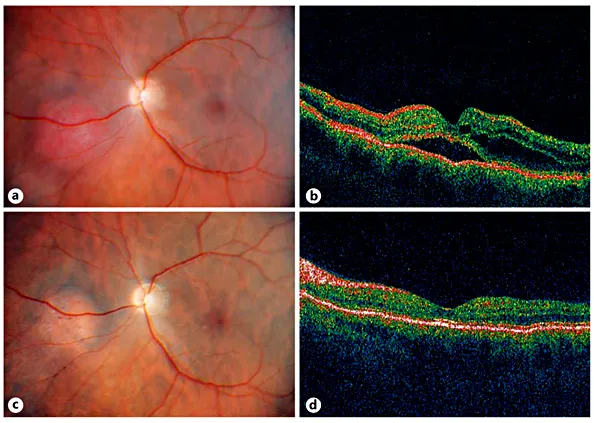
Fig. 3. Circumscribed choroidal hemangioma associated with cystoid macular edema and a serous foveolar detachment. a Panoramic color fundus picture. Nasal, superiorly located red-orange tumor touching the optic disk and surrounded by a serous retinal detachment. Note the nasal gravitational epitheliopathy. b Macular OCT. Cystoid retinal edema and serous foveal detachment.
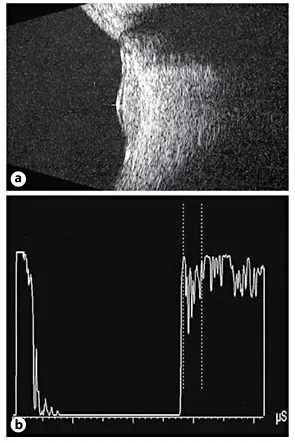
Fig. 4. Ultrasonographic examination of a circumscribed choroidal hemangioma. a B-scan ultrasonography. Small dome-shaped choroidal tumor associated with a serous retinal detachment. b A-scan ultrasonography. High internal reflectivity (92%).
F...
Table of contents
- Cover Page
- Front Matter
- Examination Techniques
- Uveal Melanocytic Tumors
- Nonmelanocytic Uveal Tumors
- Intraocular Vascular Tumors
- Intraocular Metastases
- Intraocular Lymphoma
- Retinal Pigment Epithelial Tumors
- Astrocytic Tumors
- Neuro-Oculo-Cutaneous Syndromes
- Retinoblastoma: Evaluation and Differential Diagnosis
- Retinoblastoma: Therapeutic Options
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Ocular Tumors by A. D. Singh,S. Seregard,A.D., Singh,S., Seregard, Francesco Bandello,Borja Corcóstegui,Francesco, Bandello,Borja, Corcóstegui in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Technology & Supplies. We have over one million books available in our catalogue for you to explore.