This clinical handbook is a valuable resource for any health professional who works with adolescents and young adults, whether in paediatric or adult acute care facilities or in the community. As a handbook it provides ready access to practical, clinically relevant and youth specific information.
This clinical handbook fills a clear gap, as most adolescent texts are primarily directed at paediatricians. This handbook extends its scope beyond paediatrics for three important reasons. First, many adolescents are managed by adult trained clinicians who have not had much exposure to or training in adolescent health. Secondly, the important health conditions of adolescents are often the important health conditions in young adults. Thirdly, with increased survival rates in chronic illness over the last two to three decades, it is becoming essential that clinicians in adult health care are able to assess and manage conditions that have their origins in childhood.
Each chapter is written by an expert in their field with a highly practical approach. The information is relevant and straightforward, with the aim of enhancing clinical skills.
Contents:
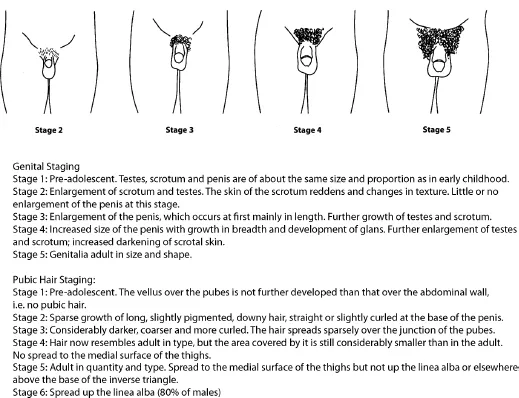
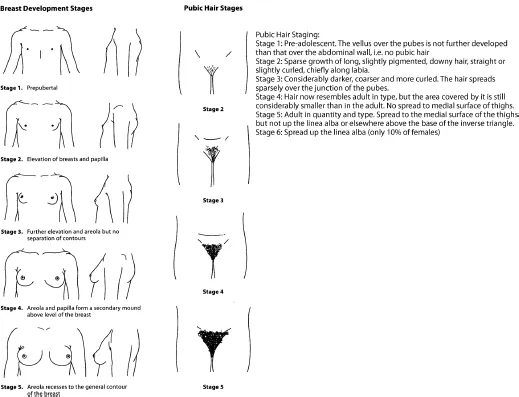
- Normal Physical Development and Growth at Puberty (Geoffrey Ambler)
- The Normal Development of the Adolescent Brain (Donna M Palmer and Leanne M Williams)
- Normal Psychosocial Development in Adolescence (David Bennett and Richard G MacKenzie)
- Body Image Issues in Adolescents (Jennifer O'Dea)
- Communicating with Adolescents (Richard G MacKenzie)
- Consent and Confidentiality (Michelle Yeo)
- Communicating with Parents and Carers (Anne Honey and Gwynneth Llewellyn)
- Communicating Electronically with Adolescents (Fiona Robards and Andrew Campbell)
- Education Issues (Margaret Allan)
- Adolescents and Young Adults in Adult Hospitals (Gail Anderson, Tegan Sturrock and Patricia Kasengele)
- Self-Management in Chronic Illness; Promoting Therapy Adherence (Michele Casey and Kate Steinbeck)
- Complex Medicopsychosocial Conditions: Chronic and Functional Disorders (Susan J Towns and Helen E Bibby)
- Transition from Paediatric to Adult Care in Chronic Illness (Sandra Whitehouse, Lynne Brodie and Susan J Towns)
- Resilience (Emily Klineberg)
- Alcohol and Other Drugs (Bronwyn Milne, Yvonne Bonomo and Gilbert Whitton)
- Unintentional Injuries Among Adolescents and Young Adults (Richard E Bélanger and Joan-Carles Suris)
- Rural and Remote Australian Adolescent Health Issues (Catherine Hawke)
- Important Medical and Mental Health Issues for Incarcerated and Homeless Youth (Stephen Stathis, Lee Hudson and Andrew Kennedy)
- The Dying Adolescent (Michael Stevens, Julie Dunsmore and John Collins)
- Disorders of Puberty (Ann Maguire and Kate Steinbeck)
- The Deaf Adolescent (Eric Weiselberg)
- The Adolescent and Young Adult with Intellectual Disability and Complex Health Needs (Helen Somerville and Cameron Ly)
- Key Issues in Adolescent Obesity (Shirley Alexander, Alison G Hoppin and Louise A Baur)
- Adolescents with Eating Disorders (Jorge L Pinzon, Gail Anderson and Simon Clarke)
- Adolescent Sexuality, Sexual and Reproductive Health (Melissa Kang, Rachel Skinner and Deborah Bateson)
- Physical Activity and Sports Medicine (Carolyn Broderick and Damien McKay)
- Depression and Anxiety (Sloane Madden)
- Assessment and Treatment of Psychotic Disorders in Adolescence (Jean Starling and Anthony Harris)
- Suicide and Self-Harm (Philip Hazell)
- Mental Health in Young People with Intellectual Disability and Autism (David Dossetor and Rameswaran Vannitamby)
- Sleep and Sleep Disorders in Adolescents (Karen Waters)
- Attention Deficit Hyperactivity Disorder (Michael R Kohn and Deborah Erickson)
- Immunisation and Infectious Diseases (Melina Georgousakis, Alexa Deirig and Robert Booy)
- Respiratory Disorders in Adolescence (Donald Payne and Siobhain Mulrennan)
- Common Adolescent Endocrine Disorders (Shubha Srinivasan)
- Diabetes During Adolescence (Kristine Heels, Nuala Harkin and Kim C Donaghue)
- Adolescent Bone Health (Craig Munns)
- Common Neurological Disorders (Richard Webster)
- Common Gastrointestinal Disorders of Adolescence (Annabel Magoffin)
- Common Dermatological Problems in Adolescents (Anuja Elizabeth George)
- Common Haematological Conditions in Adolescence (Julie Curtin)
- Allergic and Immunological Disorders in Adolescence (Alyson Kakakios, Dianne Campbell, Paul Turner and John Tan)
- Cancer in Adolescents and Young Adults (Bhavna Padhye and Melissa Gabriel)
- Late Effects of Childhood Cancer Therapy (Helena Gleeson)
- Common Cardiology Problems in Adolescence (Mugur Nicloae and Dorothy Radford)
- Adolescent Renal Medicine (Siah Kim and Deirdre Hahn)
- Common Rheumatological Conditions in Adolescence (Davinder Singh-Grewal)
- Genetics and Adolescents (David Sillence)
- Urological Problems in Adolescence (Grahame H H Smith)
- Common Gynaecological Problems in Adolescence (Kim Matthews and Peter Benny)
- The Andrology of Adolescence (David J Handelsman)
- Cardiovascular Risk Factors and Atherosclerosis (Marc S Jacobson and Michael R Kohn)
Readership: Clinicians, nurses, doctors and all other professionals in healthcare.