- 284 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
Clinical Cases for Surgery Exams
About this book
Currently, clinical training for undergraduates is becoming more difficult. To be a good doctor with adequate training, one must be exposed to many different patients with a variety of pathologies and diseases. At present, we are unable to achieve this, mainly due to the increase in the medical student cohort each year and fewer in-patients. In short, the student-to-patient ratio is worsening, thus lessening students' contact with patients and learning experience.
Fortunately, with the objective structured clinical examination (OSCE) format, undergraduate and postgraduate teaching and examination have become more efficient. This book will be very useful for students preparing for surgical OSCEs by covering the different clinical scenarios that a certain condition might present, and allowing self-testing of the questions as well as learning from the provided answers.
Contents:
- General Surgical Principles
- Trauma
- Hepatobiliary
- Colorectal
- Vascular
- Head and Neck
- Breast
- Upper GI
- Urology
- Plastic and Reconstructive Endocrine Surgery
- Paediatric Surgery
- Neurosurgery
- Orthopaedics
Readership: Undergraduate and postgraduate medical students; trainees in surgery.
Tools to learn more effectively

Saving Books

Keyword Search

Annotating Text

Listen to it instead
Information
PRINCIPLES
- What can be seen in the chest X-ray (picture A)?
- What is the most likely diagnosis and what is its definition?
- How can we manage the patient?
- What is the equipment used to assist ventilation in picture B?


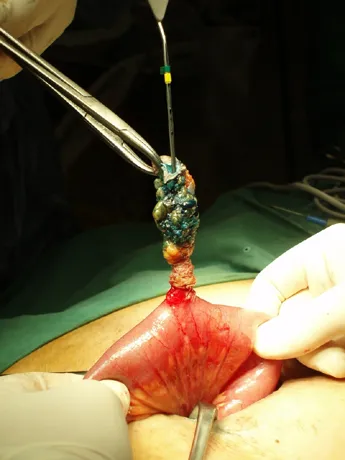
- What does this intra-operative picture show?
- What is the definition and natural history of this pathology?
- What are the possible causes of this pathology?
- What investigations can be done pre-operatively?
- What are some reasons that might prevent patients from recovering from this condition?
- There is an endo-tacheal tube in position, with a central venous catheter inserted via the right internal jugular vein and bilateral fluffy infiltrates in the lungs.
- Acute respiratory distress syndrome (ARDS) secondary to systemic sepsis.
- A known precipitating cause.
- Acute onset of symptoms.
- Hypoxia refractory to oxygen therapy.
- New, bilateral infiltrates in the CXR.
- No cardiac failure with fluid overload.
- Maximal respiratory support with removal of the primary precipitating source of sepsis, which is the liver abscess in this patient.
- Bilevel mechanical ventilatory support. It allows the patient to breathe spontaneously at two levels of positive end-expiratory pressure (PEEP).
- Isolation and excision of an enterocutaneous fistula tract. Methylene blue dye and a metallic probe are used to isolate the fistula tract so that the entire tract may be excised.
- A fistula is an abnormal communication between two epithelial-lined surfaces or viscus. In the absence of distal obstruction, most fistulas will close spontaneously.
- Trauma/injury to the bowel, Crohn's Disease, abscess, diverticulitis or an inadvertent suture left in the bowel wall after surgery.
- Computed Tomographic (CT) scans can be used to rule out an abscess collection or any inflammatory process within the fistula opening. A fistulogram may identify multiple or branched-tracts.
- High-output effluent, infection, presence of foreign material, malignancy and poor nutrition.
- What can be seen in these pictures?
- What factors may predispose one to develop the condition?
- What may be contained in this lump?
- What are the indications for emergent surgery?


- What is the condition shown in picture A?
- What would you perform to obtain more information about the patient's condition?
- What information would it provide?
- What is shown in picture B?


- Incisional hernia.
- Poor wound healing.
(patient factors) malnutrition, old age, malignancy, immunosuppression, steroids, infection, radiotherapy and obesity.
(surgeon factors) poor surgical technique and suture breakage. - Any visceral organs (most commonly small or large bowel and omentum).
- Pain, irreducibility, intestinal obstruction and peritonism which may suggest ischemia of the contents in the sac.
- Right inguinal scrotal lump.
- Attempt to “get above the lump/mass” or feel the spermatic cord.
- In adults, if you can get above the cord or feel it, then it is a scrotal or testicular mass.
If not, it is an inguinal hernia until proven otherwise. - A prosthetic mesh. There are many types of meshes available for the repair of hernias, with various shapes, sizes and materials.
After reduction of the viable contents and hernia sac, the weak posterior wall is reinforced with a tension-free deployment of the mesh. The mesh allows for the scarplate formation of the posterior wall, thus providing support to prevent the recurrence of a direct hernia.
- What has been inserted into these patients?
- What are the indications for such use?
- What two complications can be seen in pictures A and B?
- What are the other complications which may arise from such a procedure?


- What does this chest X-ray show?
- What is your diagnosis?
- What do you expect to find on clinical examination?
- What other radiological signs may be present?
- What are the possible causes of this condition?
- Outline your management.

- Central venous catheters.
- Administration of intravenous fluids or blood products.
- Monitoring i...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Dedication
- Foreword by Abu Rauff
- Foreword by Leigh Delbridge
- Preface
- Acknowledgements
- Contents
- Editors
- List of Chapter Authors
- List of Abbreviations
- 1. General Surgical Principles
- 2. Trauma
- 3. Hepatobiliary
- 4. Colorectal
- 5. Vascular
- 6. Head and Neck
- 7. Breast
- 8. Upper GI
- 9. Urology
- 10. Plastic and Reconstructive Surgery
- 11. Endocrine Surgery
- 12. Paediatric Surgery
- 13. Neurosurgery
- 14. Orthopaedics
Frequently asked questions
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.4M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app