![]()
1
Introduction to Chronic Urticaria
OVERVIEW
Chronic urticaria is defined as urticaria which lasts six weeks or more in duration. Wheals (also known as hives) are red, raised lesions which have a rapid onset, vary in size and are usually accompanied by itching (pruritus). Management with conventional medicine uses a stepped-care approach, with second-generation antihistamines as the first-line therapy. This chapter describes the various types of urticarias, pathological processes, diagnosis and management with conventional medicine.
Definition of Urticaria
Clinical Presentation and Subtypes of Chronic Urticaria
Urticaria is characterized by the development of wheals (also called hives), either alone or accompanied by angioedema.1 Wheals are red and raised in appearance,2 and vary in size from a few millimetres to several centimetres.3 Wheals have a central swelling area which is surrounded by erythema, and are usually accompanied by pruritus (itching) and/or a burning sensation. Urticaria usually resolves within 1–24 hours. If accompanied by angioedema, inflammation extends to the lower dermis and subcutis and may present with pain rather than pruritus.1 Angioedema can take up to 72 hours to resolve.
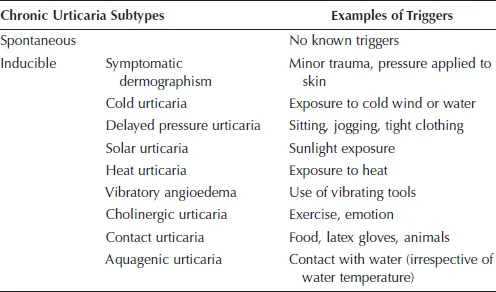
Urticaria can occur spontaneously or be induced in response to eliciting factors. Acute urticaria refers to the spontaneous onset of wheals and/or oedema which lasts less than six weeks in duration. Chronic urticaria (CU) refers to urticaria lasting six or more weeks duration, and can be categorized as either spontaneous (chronic spontaneous urticaria, CSU) or inducible.1 Symptoms can occur daily or on most days,4 or at irregular intervals.5 Clinically, CSU is not different from acute urticaria.5 Forms of chronic inducible urticaria include symptomatic dermographism, cold urticaria, delayed pressure urticaria, solar urticaria, heat urticaria, vibratory urticaria, cholinergic urticaria, contact urticaria and aquagenic urticaria (Table 1.1).1 Multiple types can co-exist within one patient at any given time.
Epidemiology
The prevalence of urticaria varies depending on duration of the condition. A German cross-sectional study found the lifetime prevalence for all types of urticaria was 8.8%. The prevalence of CU is lower, and has been reported to range from 0.5% to 5%.6 For 30–55% of patients, CU will resolve spontaneously within five years,7 although 20% may still have CSU after 20 years.3 CU is more common in women than in men;5,8 the reasons for this are uncertain. The mean age of people with all urticarias was 37.7 years,8 while mean age for chronic idiopathic (spontaneous) urticaria was 36 years.9
Table 1.1 Subtypes of Chronic Urticaria
Adapted from Zuberbier et al.1
Burden
CU has a high economic burden. In chronic idiopathic urticaria, medication costs were found to contribute 62.5% (US$1,280) of the total annual direct cost of US$2,047.10 Indirect costs such as lost wages due to outpatient appointments and work absences contributed 15.7% of total costs, although this is likely an underestimate because factors such as waiting time and costs accrued by carers and family were not accounted for. The mean annual healthcare cost was higher for women than men. Based on prevalence of 0.04% in the U.S. for chronic idiopathic urticaria, the total costs are estimated to be $244 million per year. Estimates of cost of chronic idiopathic urticaria from insurance claims found the costs of managing urticaria to be US$1,762 per year.9
The burden of urticaria is high and impacts on patients’ quality of health. The impact of CU on quality of life has been rated as similar to that of coronary artery disease, although the number of participants was small.11 Functional limitation has been reported in sleep, mobility, energy, pain, mood changes including depression, life stress, social interaction and emotional reactions.11–14 Patients with CU fared worse for sleep disruption and six of seven aspects of daily living than patients with ischaemic heart disease.11 Patients were not always aware of the level of limitation experienced as a result of urticaria.14 Impairment in quality of life measured on the Dermatology Life Quality Index (DLQI) is between 13.5%5 and 17.4%.8 The prevalence of psychosocial factors in people with CSU was 46.1%.15
Risk Factors
CU is more common in women than in men,5,8 and more common in adulthood.16
Pathological Processes
Inducible urticarias are in direct response to a trigger, and the length of time from exposure to wheal development can vary considerably, for example up to 24 hours in delayed pressure urticaria.6 Unlike inducible urticarias, there is no evidence of an allergic reaction as the cause of the disorder in CSU,17 and aetiology in urticaria generally can be difficult to establish.18
The mechanism of urticaria is complex. It is recognised as a mast-cell-driven disease, where histamine, platelet-activating factor (PAF), cytokines and other mediators are released from dermal mast cells.1 This leads to sensory nerve activation, vasodilation and extravasation of fluid and cell recruitment to urticarial lesions.1,2 There are likely to be many signals which result in mast cell activation, and currently these are not well understood. The trigger of mast cell activation is unknown.2
The most commonly accepted hypothesis is that urticaria is an autoimmune disease,19 accounting for 30–50% of CU.2 CU has been associated with other autoimmune diseases including systemic lupus erythematosus, Sjögren syndrome and Still disease,6 and the presence of thyroid antibodies are higher in people with CU.19 In urticaria of autoimmune origin, histamine-releasing autoantibodies activate immunoglobulin type E (IgE) receptors or IgE bound to receptors, stimulating degranulation of mast cells and basophils.20
The rapid release of histamine leads to vasodilatation and extravasation, which leads to pruritus.21 Histamine acts on H1-receptors on endothelial cells which results in the development of wheals, and on sensory nerves which leads to the symptoms of pruritus and neurogenic flare.1 The delayed secretion of inflammatory cytokines results in an inflammatory infiltrate at the lesion site, and longer lasting wheals.1,21 Oedema occurs in the upper and mid-dermis at the wheal site, with dilatation of postcapillary venules and lymphatic vessels in the upper dermis.1 An inflammatory infiltrate consisting of neutrophils, eosinophils, macrophages and T cells is also seen at the wheal site.
For many physical urticarias (dermographism, cold, delayed pressure, solar, heat, aquagenic), the mechanism is direct mast cell mediator release.2 In contact urticaria, wheals develop after exposure to an allergen via an IgE-mediated mechanism.2
Diagnosis
Diagnosis is made through a thorough patient history and clinical examination.1,2,6 The history should include information about the onset of the disease, frequency and duration of wheals, wheal shape, size and distribution, pr...