![]()
CHAPTER 1
Introduction
Health and wellbeing are elusive concepts and the aim of this book is to support commissioners translate current aspirations of public mental health into tangible commissioning strategies. This book provides a carefully structured and comprehensive look at the resources designed to improve population health and wellbeing outcomes. It is being published at a time when there are major changes in commissioning arrangements in England and we hope that our contribution will enable a debate within Clinical Commissioning Groups (CCGs) and Health and Wellbeing Boards (HWBs) and other emerging organisations about the possibilities for using current resources, both human and financial, by focusing on health and wellbeing as well as illness.
This chapter starts by setting the background and explains our view about positive mental health and wellbeing, making the general case for investments by health and social care commissioners in wellbeing interventions.
1.1 Introduction
The importance of mental and physical wellbeing and the positive benefits it brings to individuals and communities is now widely recognised. These include better health and health-related behaviours, greater resilience, an enhanced capacity for creativity and innovation, stronger social networks, positive relationships and connected communities as well as reduced mortality (Aked et al, 2010; DH, 2009a; National Mental Wellbeing Impact Assessment (MWIA) Collaborative, 2011). In the last six years, there have been several valuable reports published by the New Economics Foundation (nef) (see, for example, Measuring Wellbeing in Policy, 2008; Five Ways to Wellbeing: The Evidence, 2008),1 the Government Office for Science (the Foresight Report, 2008) and the Marmot Review in 2010 (Marmot, 2010). The National Institute for Health and Clinical Excellence (NICE) and the Department of Health (DH) have also published a range of reports, summarising the evidence base and promoting commissioning for mental wellbeing as a key strategic programme. Together these reports provide an evidence base for why it makes sense to focus on wellbeing and the role played by the social determinants of health, and a bibliography is available as an Appendix. The reason wellbeing has gained so much attention is the understanding that mental capital is needed to enable us to adapt to the challenges ahead, particularly to those of the global economic recession, climate change and its consequences, population growth and its effect in a reduction of resources, and greater equality between nations and continents. Even at times of austerity, an emphasis on social protection and active labour market programmes that support personal development, as well as simply getting people into a job, can encourage and promote wellbeing.
Wellbeing has become a more accepted way of understanding how people feel about the society in which they live. Since November 2010, when the Office for National Statistics (ONS) launched the Measuring National Well-being programme, a set of measures has been available that complements figures for Gross Domestic Product (GDP), offer a greater understanding of the way people feel about changes taking place in society and assist ordinary people to understand what is important to the country (ONS, 2010). Bhutan was perhaps the first country actively to consider a Gross National Happiness (GNH) quotient, but the UK may soon be catching up.2
Before we go any further, however, we need to explore what we mean by wellbeing. Although physical and mental wellbeing are inextricably linked, our focus is on mental wellbeing. Mental wellbeing is a multi-dimensional concept and is the foundation for positive health and effective functioning for an individual and for a community. We explore the concept of mental wellbeing in more detail in Chapter 2; however, the terminology is problematic and work in Scotland has found it can evoke strong emotions. There is a paradox. If we speak about ‘health’ alone, it will not be clear that we mean the totality of health-promoting psychological and physical interventions that have wellbeing as the goal; if we speak about ‘mental health’, it will not be clear that we mean comprehensive positive mental health as well as preventive strategies to reduce the risk and incidence of mental illness. We are rightly concerned with achieving positive mental health as a concomitant of a wider description of wellbeing; improvements to mental wellbeing come from improvements in physical health, and in this way physical and mental health are intimately connected. The term ‘mental health’ often, indeed usually, conjures up in the reader’s mind the idea of mental health care, or in other words mental illness services. In the discussion here we do not want to place any more than marginal emphasis on mental illness or services labelled as mental health care; our purpose is the positive mental health that stems from those aspects of society that support flourishing and resilience (see Chapter 2) whether those are social, familial, psychological, biological, organisational, economic or political determinants of wellbeing. Consequently we have called the book Commissioning Health and Wellbeing, not Mental Health and Wellbeing, hopefully for what are now obvious reasons.
In this book, we want to offer ideas that will enable commissioners to commission to achieve physical and mental health wellbeing. First, the focus will be on public (mental) health in addition to primary, secondary and tertiary prevention of any disease or distress where its course can be modified by early preventive interventions that reduce or ameliorate distress such that the long-term consequences are much improved. Second, we are concerned with cost-effective interventions in health and social care that support or improve wellbeing, for individuals, their families and communities. Third, we are concerned with the health and wellbeing of specific populations whose situation and social processes further disadvantage them and increase their vulnerability to poor health. Inevitably this includes people with a diagnosis of mental illness and so we are also concerned with interventions that will assist with recovery of service users towards the objectives they set themselves for their lives. We are not concerned with mental health care (mental illness services) except where these impinge on the generic promotion and prevention agenda; but we are interested in commissioning health and social care that promotes wellbeing, applying lessons from the literature wisely and correctly to achieve savings and longer-term benefits for wider society.
1.2 Improving health and wellbeing
Mental health as a positive concept is a key element of what we mean by health and wellbeing. Perhaps mental wellbeing might be a better term. Wellbeing is a broad construct that encompasses a variety of theoretical approaches including eudaimonic wellbeing, hedonic wellbeing, and social wellbeing (Gallagher et al., 2009). Whatever term we use though, mental health is an essential component of general health. In other words there is no health without mental health (Royal College of Psychiatrists, 2010). Mental wellbeing is a critical asset in the fight for improved health – it is both an objective and a support on the road to that objective. This means it is a resource both at an individual level, enabling people to cope with the demands of everyday living and the unexpected – in other words it is concerned with resilience – and at a social level, fostering stronger and sustainable social relationships and communities. It is a resource for the long-term social and economic prosperity of society.
In contrast to psychological ‘ill-being’ (i.e. pervasive negative feelings and poor functioning in life), positive psychological wellbeing (PPW) reflects the positive components of psychological health that characterise individuals who feel good about life and function well (Keyes and Annas, 2009; in contrast to Kashdan et al., 2008 with whom this paper disagrees. See also Tiberius and Plakias, 2010). Improving mental wellbeing requires efforts to be focused on promoting wellbeing for communities and individuals and on those at risk of poor mental health: communities, social networks and the environment play a central role alongside education, transport, health and social services, employment, financial security and leisure opportunities in strengthening resilience both at an individual and a community level. Responsibility for promoting mental wellbeing extends across all disciplines and government departments and encompasses a concern for social values, culture, economic and social, as well as health policies. It includes approaches that involve and strengthen the active participation of local communities and local people, particularly those from vulnerable groups, who are central to improving mental wellbeing. Consequently, commissioning for mental wellbeing should be focused on delivering the best possible health and wellbeing outcomes through the best use of the available information and resources.
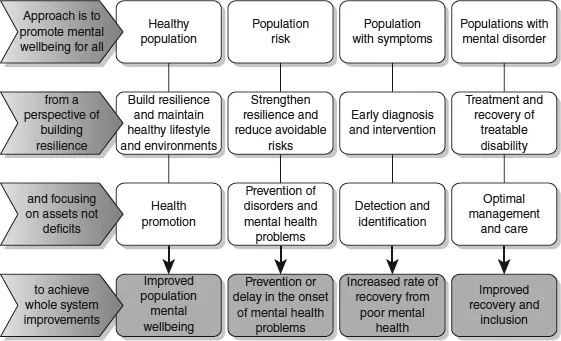
Commissioning for mental wellbeing involves considering three sets of objectives: health and wellbeing promotion for the whole population; primary, secondary and tertiary prevention of potential health and social risks; and wellbeing developments for those living with or recovering from mental illness. The Figure 1.1 summarises this approach and provides a useful framework for developing a strategic approach to commissioning for mental wellbeing. The first three columns are the focus for this book – positive wellbeing for all; prevention; and promoting health for those with incipient or actual mental health problems – but the last column is not within the remit of the book as that describes mental health services. However, this is an important area for commissioners, who will be concerned to commission mental health services that promote recovery and wellbeing.
1.3 Commissioning for outcomes
At a time of austerity it may seem naïve, even foolish, to suggest health promoting and preventive interventions; yet there is a strong case to be made on the basis of the evidence available for a range of outcomes including social and economic ones. Improving population mental wellbeing has the potential to contribute to far-reaching improvements in physical and mental health, a better quality of life, higher educational attainment, economic wellbeing and reduction in crime and anti-social behaviour. The main outcomes, which have been well evidenced, are illustrated in Box 1.1 (see, for example, Kim-Cohen et al., 2003; Saxena et al., 2006; Barry and Jenkins, 2007; Friedli and Parsonage, 2007).
The foundations for positive mental wellbeing are laid down in early life and as we grow and mature through our teenage years. This is when we learn most rapidly. The quality of the relationships and experiences we have in our early years and the learning that we do about our emotions and our relationships as we grow up are vital. For example, half of lifetime mental illness (excluding dementia) is already present by the age of 14 (Kessler et al., 2005) so the early years provide a critical opportunity for intervention. Mental wellbeing is important across the life span and the health and wellbeing of older generations affects that of younger people. Thus, better outcomes are likely to be achieved through the adoption of a life course approach that recognises that mental capital, as discussed in Chapter 2, is a resource we develop and use throughout our life and is available to and built by others, reflecting our interdependencies and interconnectedness.
Box 1.1 Advantages and outcomes of focusing on health and wellbeing
• Increased quality of life and overall wellbeing.
• Increased life expectancy, provide protection from coronary heart disease, improve health outcomes from a range of long-term conditions (e.g. diabetes).
• Reduce risks to health through influencing positive health behaviours, such as reductions in alcohol and substance use.
• Reduced health inequalities – both physical and mental health – and impact positively on the social determinants of health.
• Improved educational attainment, outcomes and subsequent occupation.
• Safer communities with less crime.
• Improved productivity and employment retention, reduced sickness absence from work and reduced ‘presenteeism’.
• Reduced levels of poor mental health and mental illness and the adverse consequences of mental illness or distress (NB wellbeing is not the opposite of mental illness).
1.4 The case for commissioning for mental wellbeing
Current health (NHS) and local authorities’ policy is that commissioning for health, wellbeing and independence3 is as important as commissioning for ‘illness’ (see, for example, North Yorkshire County Council, 2007; Bennett et al., 2011; DH, 2011a). This emphasis includes a growing awareness of the negative impact of poor mental wellbeing and indeed poor mental health, as well as opportunities for intervention at a population and individual level. The case for mental wellbeing improvement is an increased quality of life and overall wellbeing, and wider health benefits to individuals and the population. Mental wellbeing ...