![]()
1
THEORIES AND MODELS
NOVA CORCORAN
Learning objectives:
- Define the term ‘communication’ and identify components of the communication process in a health promotion context.
- Explore communication theory in relation to health promotion practice.
- Apply theoretical models of health promotion to the health promotion and health education setting.
Communication has an essential role in any action that aims to improve and promote health. New models of communication recognise that the communication process involves a multi-way interaction between the sender and receiver of health messages. This chapter will define the communication process and consider four behaviour change models that can be applied in successful campaign and communication design. This includes emphasis on how communication is disseminated through populations as well as influential factors in the communication process. This chapter seeks to bridge the theory to practice gap and emphasises the application of theoretical models to practice.
COMMUNICATION DEFINED
Communication is a transactional process and in a health context it is an important part of health promotion work. It is vital in the achievement of healthy individuals and populations and contributes to the reduction in inequalities. Health communication is understood as ‘an enabler of individual and social levels change to achieve established development goals including health’ (Suresh, 2011:276).
The communication transaction is one of sharing information using a set of common rules (Northouse and Northouse, 1998). In health promotion communication is a process that is essential in the achievement of health outcomes. Communication is usually a process that comes to fruition when the audience has achieved, acted on or responded to messages that ultimately aim to increase health goals.
COMPONENTS OF COMMUNICATION
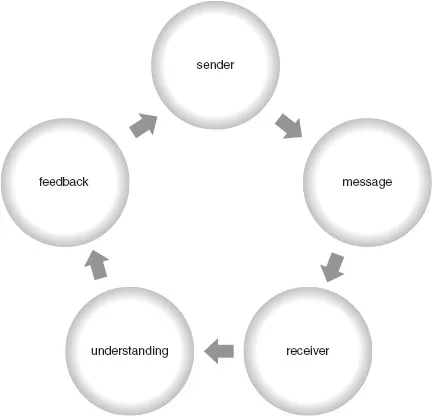
Historically the basic representative model of communication was usually conceptualised as a one-way flow process consisting of a sender, message and receiver. More recent work in the area of communication added fourth and fifth variables: complete understanding by that receiver and feedback to the communicator. These last two variables hold importance to health communication as they imply two-way communication, enabling a move away from the traditional concept of oneway communication towards multi-way communication. Communication is a cyclic process involving a series of actions, thus a modified model can be represented as circular (see Figure 1.1).
Figure 1.1 A multi-way model of communication
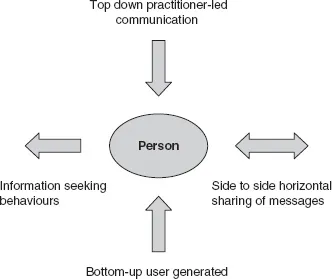
Figure 1.2 A new model of communication, adapted from Thackeray and Neiger (2009)
The most recent developments in health communication reflect the evolving notion that the health communication process is multidirectional as the general population actively seek information from the immediate, accessible formats available to them, for example from the Internet. This has created a model of communication that is no longer an expert-driven top-down model of communication, but a non-hierarchical, horizontal form of communication. Thackeray and Neiger (2009) also concur with this idea and suggest a communication model which emphasises this bottom-up and horizontal approach. This model is represented in Figure 1.2.
This model assumes that communication can be expert-generated from both the top down but also from the bottom up, and therefore user-generated as well as side-to-side sharing (horizontal). It is suggested that effective health communication must involve an active collaborative transaction between the sender and receiver (Kreps and Neuhauser, 2010). This view emphasises that in order for a change to occur, i.e. in a health behaviour, the receiver must take more of a proactive part in the communication process instead of passively receiving messages.
FACTORS INFLUENCING COMMUNICATION
The multidimensional and dynamic nature of communication means that transactions contain other aspects that influence communication. Watzlawick et al. (1967) break communication down into ‘content’ and ‘relationship’. The ‘content’ includes the message, the words and the information transmitted. The ‘relationship’ consists of the dynamics between those involved in the communication transaction – the communicator(s). This breakdown has the advantage of identifying the content and the relationship between the sender and receiver separately. In Communicating Health: Strategies for health promotion the main sender is the health practitioner and the receiver is the intended audience (who will be discussed in more detail in Chapter 2). Traditionally the relationship between the sender and receiver is defined as horizontal, but as the main focus of this textbook is for the practitioner to develop skills in communication the sender is essentially going to be a health practitioner. The content aspect is currently of considerable interest in this chapter.
The content of a message contains verbal and non-verbal communication. Verbal communication is the words, sentences and phrases used (Minardi and Riley, 1997). Non-verbal communication, according to Ellis and Beattie (1986), contains the four elements of prosodic, paralinguistic, kinesics and standing features:
- Prosodic elements include intonation and rhythm. These can influence how the sender delivers the message and the receiver interprets it. For example, comprehension would alter if the sender of a message spoke quickly or slowly.
- Paralinguistic features include vocal but non-verbal expressions like ‘mmm’ or ‘ahhh’. These can alter the way messages are communicated, particularly in relation to the prosodic features described above.
- Kinesic elements include body language, eye contact, posture or gestures. For example, different interpretations of messages would be transmitted by a sender who was trying to maintain eye contact as opposed to a sender who was looking at their feet.
- Standing features include factors such as appearance. Some people have preconceived notions of what practitioners who deliver health information should look like. This can include their dress, gender, ethnic group and other appearance-related factors.
Language and lexical content of the message is also important. Lexical content, which literally means the words, can be used positively or negatively. Using words from complex medical technology or abbreviating key terms can confuse messages and exclude the target audience, whereas repetition has been positively found to influence communication (Pechmann and Reibling, 2000).
As a health practitioner, the communication method will alter the importance of additional factors such as lexical content and body language. The communication process will dictate the aspects that are the most important. If you are sending every house in one area an information document about prevention of food-related illness and hence have minimal contact with the client group, your appearance and eye contact will be of little importance. If you are delivering a brief one-to-one intervention on stopping smoking in a health care setting your verbal communication, eye contact or appearance will be important.
COMMUNICATION IN HEALTH PROMOTION
Communication in health takes place on many constructs, including individual, group, community or mass media. Communication in health can be defined in much the same way as communication has generally been defined: a transactional process. Kreps (2003) summarises the addition of ‘health’ to the definition of the term communication as a ‘resource’ that allows health messages (e.g. prevention or awareness) to be used in the education and avoidance of ill health. This broad definition incorporates the fact that health communication can take place at many levels.
ACTIVITY 1.1
How are health promotion messages communicated?
There are a number of ways (or ‘mediums’) that can be used for communicating messages. Many of these can be used in communicating health messages.
- Think of as many ways of communicating information as you can.
- Which methods are most popularly used in communicating health promotion messages?
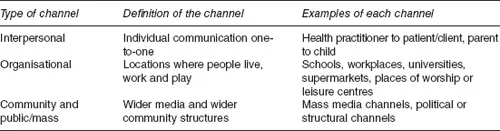
There are a range of communication channels that usually fall into four categories: interpersonal, organisational, community and public/mass. These are hierarchical in nature with interpersonal (one-to-one communication) reaching the least amount of people, and community reaching the whole population. Outside these channels are a variety of approaches which practitioners may use to achieve their goals. These include strategic communication, behaviour change communication, advocacy and social mobilisation. These methods are discussed in more detail in Chapter 2. Figure 1.3 illustrates these hierarchical channels. ‘Interpersonal’ communication is communication on a personal level. This includes one-to-one communication or small group communication. ‘Organisational’ communication includes communication in an organisation, both formal and informal. ‘Community’ communication includes media that are used in community settings, for example local radio and newspapers. ‘Public/mass’ communication is large-scale and includes national and international communication. Current research suggests that combining both interpersonal communication with communication at organisational or community level is more effective that mass media alone (see Chapter 4). Different health needs and priorities will require different styles of communication. For example, building negotiation skills for safer sex is more likely to be achieved through an interpersonal approach. Challenging incorrect beliefs about HIV transmission could be achieved through a community approach. It has been noted however that this may not always be the case, for example those who are socially isolated and have limited social networks are less likely to use interpersonal communication and use mediated channels, i.e. television instead (Askelson et al., 2011), suggesting that hard-to-reach groups may be excluded from the more direct interpersonal communication channels.
Figure 1.3 Channels of communication examples
MODELS AND THEORIES OVERVIEW
The UK government Choosing Health: Making healthy choices easier White Paper (DH, 2004) identifies one fundamental and important problem with health messages: that it is not a lack of information in health, but that it is ‘inconsistent, uncoordinated and out of step’ (DH, 2004: 21) with the way the population live their lives. This suggests perhaps that despite efforts from health practitioners, some messages are not as effective as they could be. Other authors argue that health practitioners can no longer provide knowledge, materials and support and assume the message will be sufficient for a behaviour change (Achterberg et al., 2010).
The Population Reference Bureau (2005) in the US suggests that human behaviour is the central factor in most leading causes of mortality and morbidity. They advocate that behaviour change strategies should be at the forefront of any attempts to reduce mortality and morbidity. Being able to predict behaviour makes it easier to plan an intervention (Naidoo and Wills, 2009). Therefore the first stage of any communication campaign is to analyse the behavioural aspects of the health problem (Atkin, 2001).
In addition it is proposed that if we can understand factors that influence behaviour ‘we will be in a better position to devise strategies and formulate methods that will achieve our health education goals – no matter what our philosophy or what model we choose to follow’ (Tones and Tilford, 1994: 83). Theory enables the practitioner to predict the outcomes of interventions and th...